

Eculizumab Use for Kidney Transplantation in Patients With a Diagnosis of Atypical Hemolytic Uremic Syndrome
- PMID: 30899871
- PMCID: PMC6409407
- DOI: 10.1016/j.ekir.2018.11.010
Eculizumab Use for Kidney Transplantation in Patients With a Diagnosis of Atypical Hemolytic Uremic Syndrome
Abstract
Introduction: Recurrence of atypical hemolytic uremic syndrome (aHUS) in renal allografts is common, leading to dialysis and graft failure. Pretransplant versus posttransplant initiation of eculizumab treatment in patients with aHUS has not been rigorously investigated. We hypothesized eculizumab pretransplant would reduce dialysis incidence posttransplant.
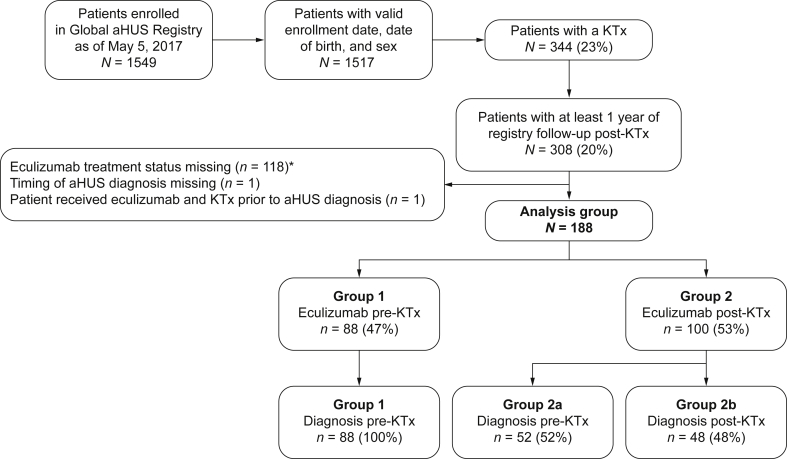
Methods: Of patients enrolled in the Global aHUS Registry (n = 1549), 344 had ≥1 kidney transplant. Of these, 188 had received eculizumab. Eighty-eight patients (47%) were diagnosed with aHUS and received eculizumab before, and during, their most recent transplant (group 1). A total of 100 patients (53%; group 2) initiated eculizumab posttransplantation. This second group was subdivided into those diagnosed with aHUS before (n = 52; group 2a) or after (n = 48; group 2b) their most recent transplant.
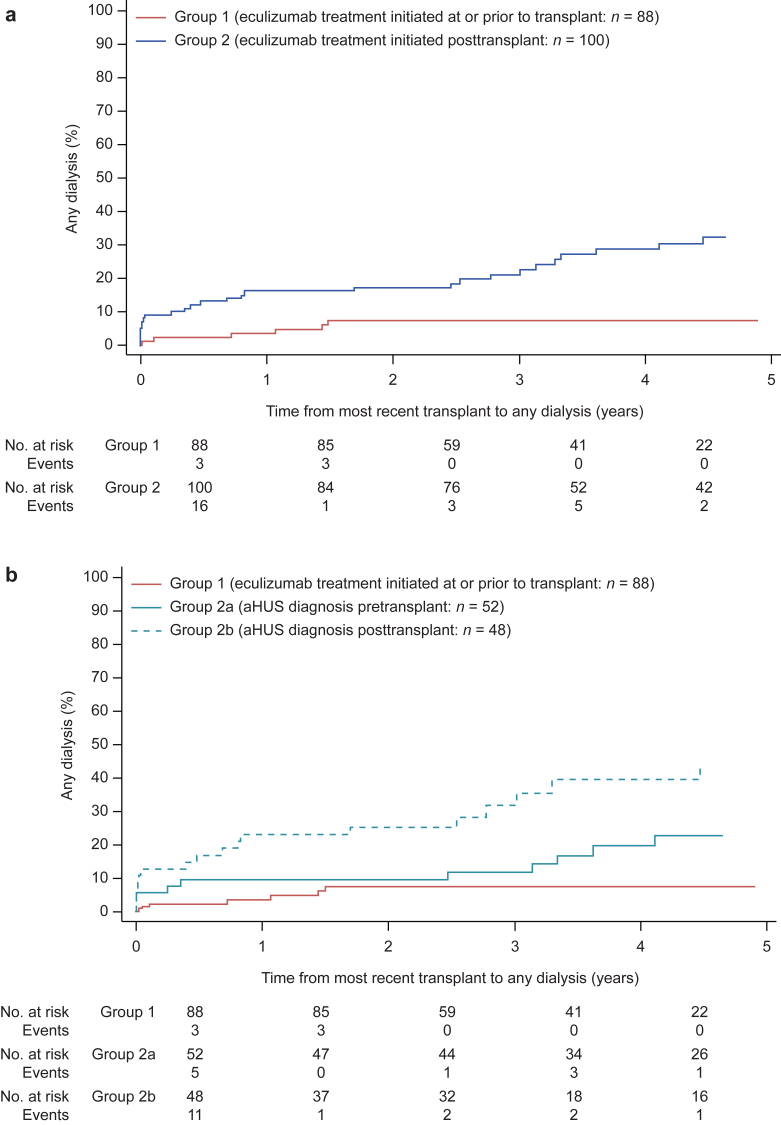
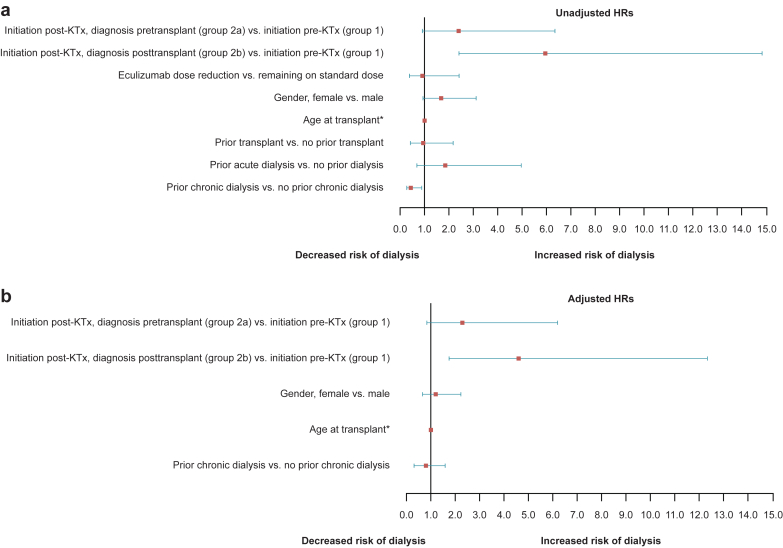
Results: Within 5 years of transplantation, 47 patients required dialysis; the risk of dialysis after transplantation was significantly increased in group 2b (hazard ratio [HR] 4.6; confidence interval [CI] 1.7-12.4) but not 2a (HR 2.3; CI 0.9-6.2). Graft function within 6 months of transplantation was significantly better in group 1 (median estimated glomerular filtration rate of 60.6 ml/min per 1.73 m2) compared with 31.5 and 9.6 ml/min per 1.73 m2 in groups 2a (P = 0.004) and 2b (P = 0.0001), respectively. One meningococcal infection (resolved with treatment) and 3 deaths (deemed unrelated to eculizumab) were reported.
Conclusions: Outcomes for transplant patients with aHUS treated with eculizumab were improved compared with previous reports of patients with aHUS not treated with eculizumab. Our findings suggest delayed aHUS diagnosis and therefore treatment is associated with an increased risk of dialysis posttransplantation and reduced allograft function.
Keywords: atypical hemolytic uremic syndrome; dialysis; eculizumab; kidney observational study; transplantation.
Figures




References
-
- Le Quintrec M., Zuber J., Moulin B. Complement genes strongly predict recurrence and graft outcome in adult renal transplant recipients with atypical hemolytic and uremic syndrome. Am J Transplant. 2013;13:663–675. - PubMed
-
- Zuber J., Le Quintrec M., Krid S. Eculizumab for atypical hemolytic uremic syndrome recurrence in renal transplantation. Am J Transplant. 2012;12:3337–3354. - PubMed
-
- Legendre C.M., Licht C., Muus P. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368:2169–2181. - PubMed
-
- Greenbaum L.A., Fila M., Ardissino G. Eculizumab is a safe and effective treatment in pediatric patients with atypical hemolytic uremic syndrome. Kidney Int. 2016;89:701–711. - PubMed
LinkOut - more resources
Full Text Sources
