

Hippocampus subfield volumetry after microsurgical or endovascular treatment of intracranial aneurysms-an explorative study
- PMID: 30900111
- PMCID: PMC6428873
- DOI: 10.1186/s41747-019-0092-7
Hippocampus subfield volumetry after microsurgical or endovascular treatment of intracranial aneurysms-an explorative study
Abstract
Background: To study hippocampus subfield volumes in patients after microsurgical clipping (MC) and/or endovascular coiling (EC) of intracranial aneurysms.
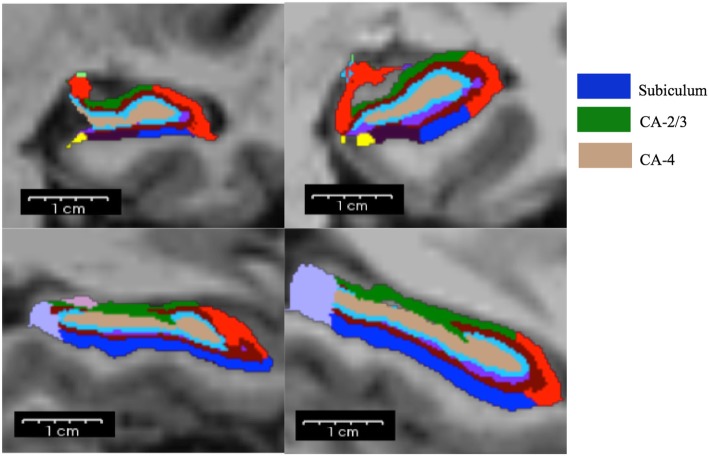
Methods: Hippocampus subfield volumetry was performed using FreeSurfer v6.0 in 51 patients (35 females, mean age 54.9 ± 11.9 years, range 24-78 years). Visual inspection of image and segmentation quality was performed prior to statistical analyses. Multiple regression analysis, controlled for age, sex, and side of treatment, was used to assess the impact of prior MC and history of subarachnoid haemorrhage (SAH) on hippocampus subfield volumes (cornu ammonis (CA)-2/3, CA-4, subiculum). Partial correlation analyses were used to assess effect of multiple treatments on hippocampus subfield volumes.
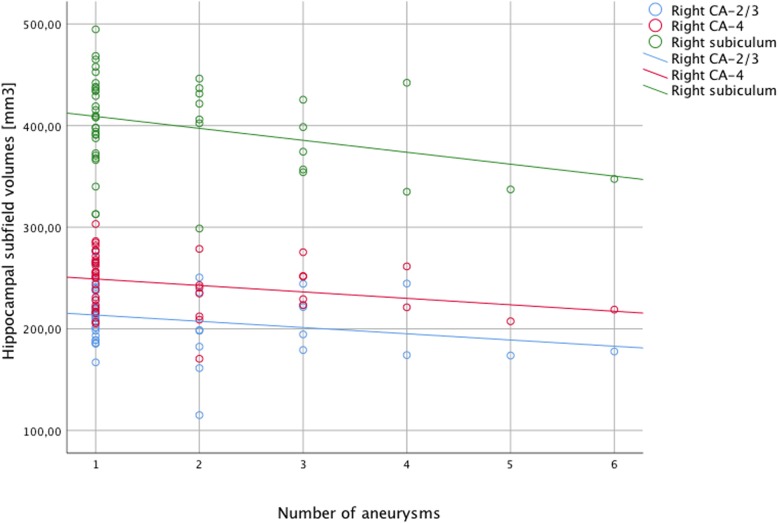
Results: Prior MC was significantly associated with lower hippocampal subfield volumes in MC patients for right and left CA-2/3 (β = -22.32 [-40.18, -4.45]; p = 0.016 and β = -20.03 [-39.38, -0.68]; p = 0.043) and right CA-4 (β = -17.00 [-33.86, 0.12]; p = 0.048). History of SAH was not significantly associated with hippocampal subfield volumes. We observed a higher disease burden in the MC cohort. The number of aneurysms correlated with right-sided hippocampal subfield volumes while the number of treatment interventions did not.
Conclusion: In this explorative study, we found that history of MC was significantly associated with lower volumes in distinct hippocampal subfields, which may be a consequence of a more extensive treatment. This could indicate specific atrophy of CA-2/3 after MC and should motivate hippocampal subfield assessment in larger cohorts.
Keywords: Intracranial aneurysm, Hippocampus, Magnetic resonance imaging, Radiology (interventional).
Conflict of interest statement
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Approval by the ethics committee was given in 03/2012 under project number 5295/12.
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- von Vogelsang AC, Forsberg C, Svensson M, Wengström Y (2015) Patients experience high levels of anxiety 2 years following aneurysmal subarachnoid hemorrhage. World Neurosurg 83:1090–1097. - PubMed
-
- Al-Khindi T, MacDonald RL, Schweizer TA (2010) Cognitive and functional outcome after aneurysmal subarachnoid hemorrhage. Stroke 41:519–536. - PubMed
-
- Ruan C, Long H, Sun H et al (2015) Endovascular coiling vs. surgical clipping for unruptured intracranial aneurysm: a meta-analysis. Br J Neurosurg 29:485–492. - PubMed
-
- Wenz H, Wenz R, Ehrlich G, Groden C, Schmieder K, Fontana J (2015) Patient characteristics support unfavorable psychiatric outcome after treatment of unruptured intracranial aneurysms. Acta Neurochir (Wien) 157:1135–1145. - PubMed
LinkOut - more resources
Full Text Sources