

All about portal vein: a pictorial display to anatomy, variants and physiopathology
- PMID: 30900187
- PMCID: PMC6428891
- DOI: 10.1186/s13244-019-0716-8
All about portal vein: a pictorial display to anatomy, variants and physiopathology
Abstract
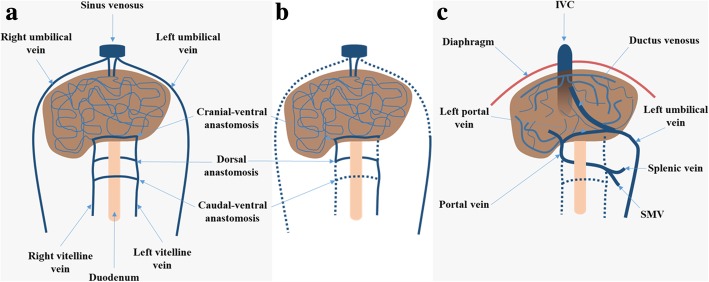
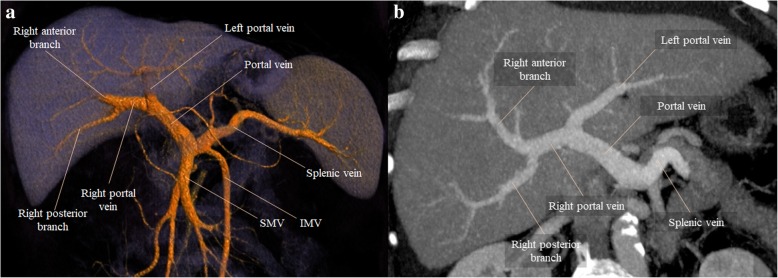
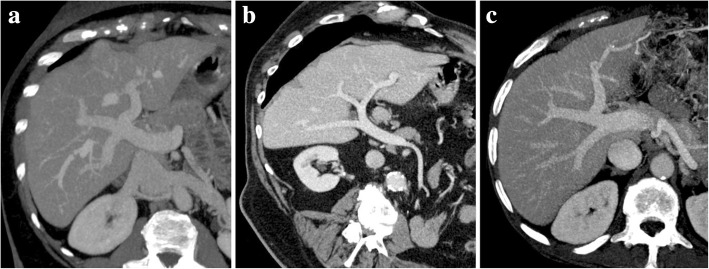
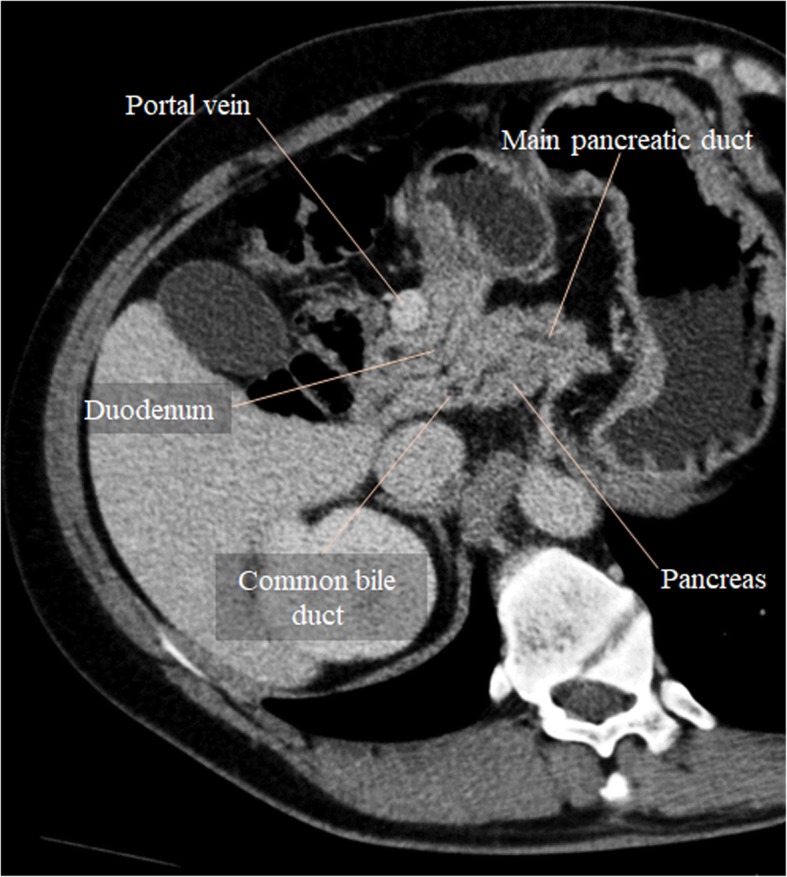
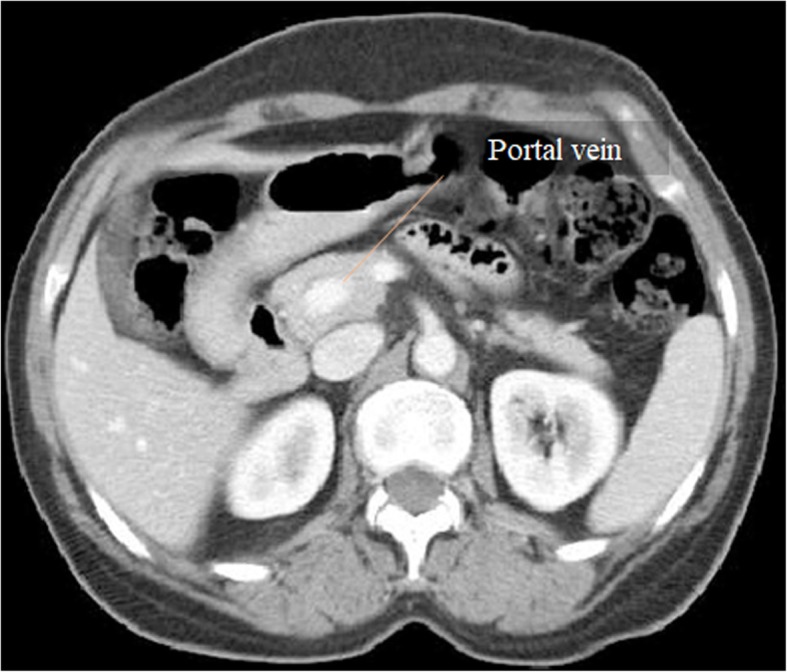
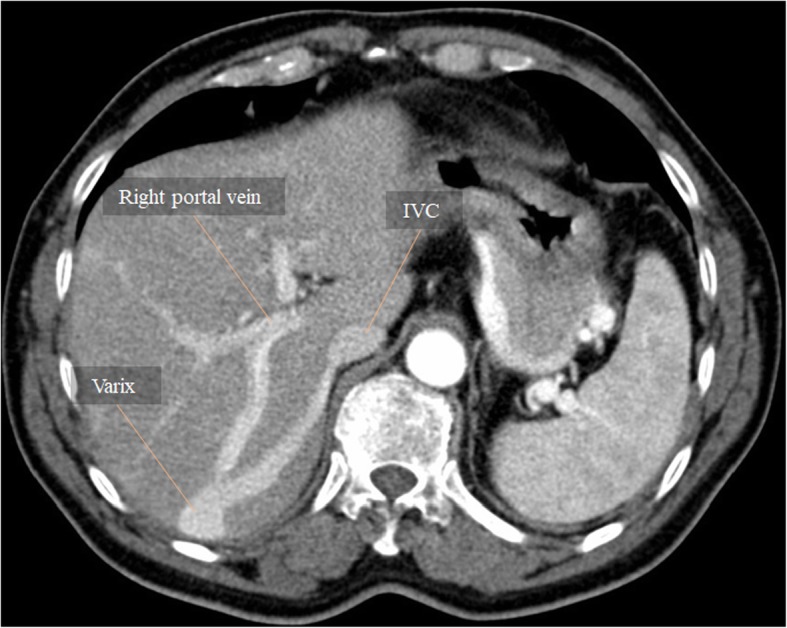
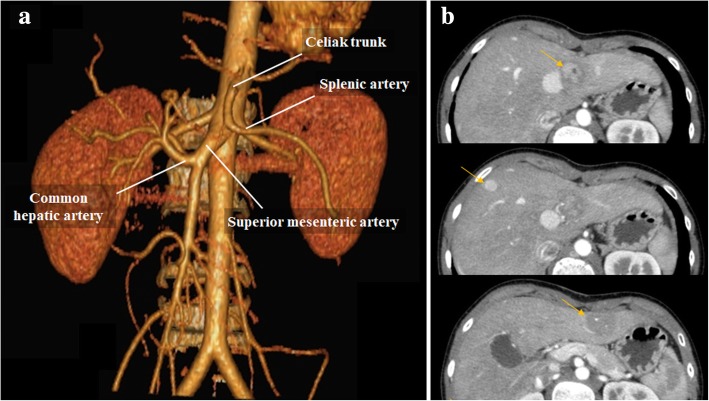
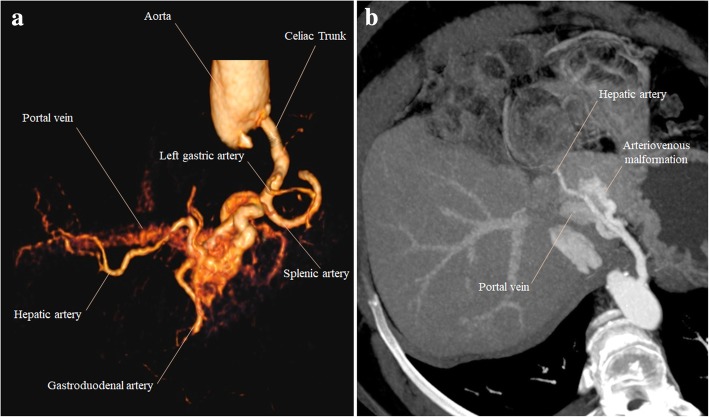
The portal vein (PV) is the main vessel of the portal venous system (PVS), which drains the blood from the gastrointestinal tract, gallbladder, pancreas, and spleen to the liver. There are several variants affecting the PV, and quite a number of congenital and acquired pathologies.In this pictorial review, we assess the embryological development and normal anatomy of the PVS, displaying selected cases consisting of normal variants, congenital anomalies, and a large and heterogeneous group of acquired conditions that may affect the PV.
Keywords: Anatomic variation; Portal hypertension; Portal system; Portal vein; Venous thrombosis.
Conflict of interest statement
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures





References
-
- Lee WK, Chang SD, Duddalwar VA et al (2011) Imaging assessment of congenital and acquired abnormalities of the portal venous system. Radiographics 31:905–926 - PubMed
-
- Mihai F, Bar C, Savin ML, Cucuteanu B, Negru D (2011) CT appearance of collateral pathways in portal hypertension. 10.1594/ecr2011/C-0972
-
- Covey AM, Brody LA, Getrajdman GI, Sofocleous CT, Brown KT (2004) Incidence, patterns, and clinical relevance of variant portal vein anatomy. AJR Am J Roentgenol 183:1055–1064 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
