

Efficacy and safety of tofacitinib for the treatment of rheumatoid arthritis in patients from the Asia-Pacific region: Post-hoc analyses of pooled clinical study data
- PMID: 30900375
- PMCID: PMC6617812
- DOI: 10.1111/1756-185X.13516
Efficacy and safety of tofacitinib for the treatment of rheumatoid arthritis in patients from the Asia-Pacific region: Post-hoc analyses of pooled clinical study data
Abstract
Aim: We report tofacitinib efficacy and safety in Asia-Pacific patients who participated in the rheumatoid arthritis (RA) clinical development program.
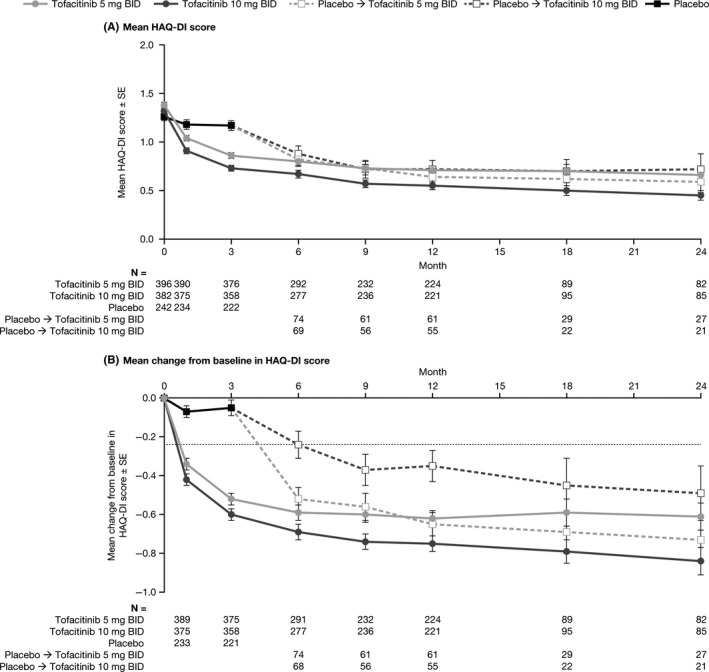
Method: This post-hoc analysis included pooled data from patients with RA in the Asia-Pacific region treated with tofacitinib with/without conventional synthetic disease-modifying antirheumatic drugs in Phase (P)1, 2, 3, and long-term extension (LTE) studies (one LTE ongoing; January 2016 data-cut). Efficacy was assessed over 24 months in patients who received tofacitinib 5 (N = 397) or 10 (N = 382) mg twice daily or placebo (N = 243) in three P2 and five P3 studies. Endpoints included American College of Rheumatology (ACR)20/50/70 responses, Disease Activity Score in 28 joints, erythrocyte sedimentation rate (DAS28-4[ESR]) and Clinical Disease Activity Index (CDAI) remission rates, and change from baseline in Health Assessment Questionnaire-Disability Index (∆HAQ-DI). Safety data pooled over 92 months from one P1, four P2, six P3, and two LTE studies for all tofacitinib doses (N = 1464) included incidence rates (IRs) (patients with events/100 patient-years) for adverse events (AEs) of special interest.
Results: At month 3, patients receiving tofacitinib 5/10 mg twice daily improved vs placebo in ACR20 (69.2%/77.9% vs 27.5%), ACR50 (36.9%/44.4% vs 9.5%), and ACR70 (15.1%/22.4% vs 2.7%) responses, remission rates for DAS28-4(ESR) (8.5%/18.5% vs 2.6%) and CDAI (6.1%/12.3% vs 0.5%), and ∆HAQ-DI (-0.5/-0.6 vs -0.1); improvements were sustained through 24 months. IRs (95% CI) were 9.4 (8.5, 10.3) for serious AEs, 9.1 (8.3, 10.1) for discontinuations due to AEs, 3.7 (3.2, 4.3) for serious infections, 5.9 (5.2, 6.7) for herpes zoster, and 0.8 (0.6, 1.1) for malignancies (excluding non-melanoma skin cancer).
Conclusion: In Asia-Pacific patients, tofacitinib improved signs/symptoms over 24 months. Safety over 92 months was generally consistent with global tofacitinib studies; however, infection IRs were higher in Asia-Pacific patients.
Keywords: clinical aspects; drug treatment; rheumatoid arthritis.
© 2019 The Authors. International Journal of Rheumatic Diseases published by Asia Pacific League of Associations for Rheumatology and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
EBL is a consultant for Pfizer Inc, and received a research grant from Green Cross Co, Republic of Korea. YL has nothing to disclose. W‐CT has received speaking or consultant fees from Abbott, AstraZeneca, Bristol‐Myers Squibb, Chugai, Janssen, Mitsubishi Tanabe, Pfizer Inc and Roche. HY has received research grants from AbbVie, Astellas, Ayumi, Bristol‐Myers Squibb, Chugai, Daiichi Sankyo, Eisai, Kaken, Mitsubishi Tanabe, MSD, Nippon Shinyaku, Ono, Pfizer Inc, Takeda, Teijin, Torii and UCB; and has received lecturing or consulting fees from Astellas, Bristol‐Myers Squibb, Chugai, Daiichi Sankyo, Mitsubishi Tanabe, Nippon Kayaku, Pfizer Inc, Takeda, Teijin and YL Biologics. CC, KK, LJL, YL, NS, LW and H‐JY are employees and shareholders of Pfizer Inc. YT has received consulting and speaking fees from Astellas, Bristol‐Myers Squibb, Chugai, Daiichi Sankyo, Eli Lilly, Janssen, Mitsubishi Tanabe, Pfizer Inc, Sanofi, UCB and YL Biologics.
Figures


References
-
- Cross M, Smith E, Hoy D, et al. The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1316‐1322. - PubMed
-
- Kremer JM, Bloom BJ, Breedveld FC, et al. The safety and efficacy of a JAK inhibitor in patients with active rheumatoid arthritis: results of a double‐blind, placebo‐controlled phase IIa trial of three dosage levels of CP‐690,550 versus placebo. Arthritis Rheum. 2009;60(7):1895‐1905. - PubMed
-
- Tanaka Y, Suzuki M, Nakamura H, Toyoizumi S, Zwillich SH; Tofacitinib Study Investigators . Phase II study of tofacitinib (CP‐690,550) combined with methotrexate in patients with rheumatoid arthritis and an inadequate response to methotrexate. Arthritis Care Res (Hoboken). 2011;63(8):1150‐1158. - PubMed
-
- Fleischmann R, Cutolo M, Genovese MC, et al. Phase IIb dose‐ranging study of the oral JAK inhibitor tofacitinib (CP‐690,550) or adalimumab monotherapy versus placebo in patients with active rheumatoid arthritis with an inadequate response to disease‐modifying antirheumatic drugs. Arthritis Rheum. 2012;64(3):617‐629. - PubMed
-
- Kremer JM, Cohen S, Wilkinson BE, et al. A phase IIb dose‐ranging study of the oral JAK inhibitor tofacitinib (CP‐690,550) versus placebo in combination with background methotrexate in patients with active rheumatoid arthritis and an inadequate response to methotrexate alone. Arthritis Rheum. 2012;64(4):970‐981. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
