Rates of Extreme Neonatal Hyperbilirubinemia and Kernicterus in Children and Adherence to National Guidelines for Screening, Diagnosis, and Treatment in Sweden
- PMID: 30901042
- PMCID: PMC6583272
- DOI: 10.1001/jamanetworkopen.2019.0858
Rates of Extreme Neonatal Hyperbilirubinemia and Kernicterus in Children and Adherence to National Guidelines for Screening, Diagnosis, and Treatment in Sweden
Abstract
Importance: Neonatal hyperbilirubinemia can cause lifelong neurodevelopmental impairment (kernicterus) even in high-resource settings. A better understanding of the incidence and processes leading to kernicterus may help in the design of preventive measures.
Objectives: To determine incidence rates of hazardous hyperbilirubinemia and kernicterus among near-term to term newborns and to evaluate health care professional adherence to best practices.
Design, setting, and participants: This population-based nationwide cohort study used prospectively collected data on the highest serum bilirubin level for all infants born alive at 35 weeks' gestation or longer and admitted to neonatal care at all 46 delivery and 37 neonatal units in Sweden from 2008 to 2016. Medical records for newborns with hazardous hyperbilirubinemia were evaluated for best neonatal practices and for a diagnosis of kernicterus up to 2 years of age. Data analyses were performed between September 2017 and February 2018.
Exposures: Extreme (serum bilirubin levels, 25.0-29.9 mg/dL [425-509 μmol/L]) and hazardous (serum bilirubin levels, ≥30.0 mg/dL [≥510 μmol/L]) neonatal hyperbilirubinemia.
Main outcomes and measures: The primary outcome was kernicterus, defined as hazardous neonatal hyperbilirubinemia followed by cerebral palsy, sensorineural hearing loss, gaze paralysis, or neurodevelopmental retardation. Secondary outcomes were health care professional adherence to national guidelines using a predefined protocol with 10 key performance indicators for diagnosis and treatment as well as assessment of whether bilirubin-associated brain damage might have been avoidable.
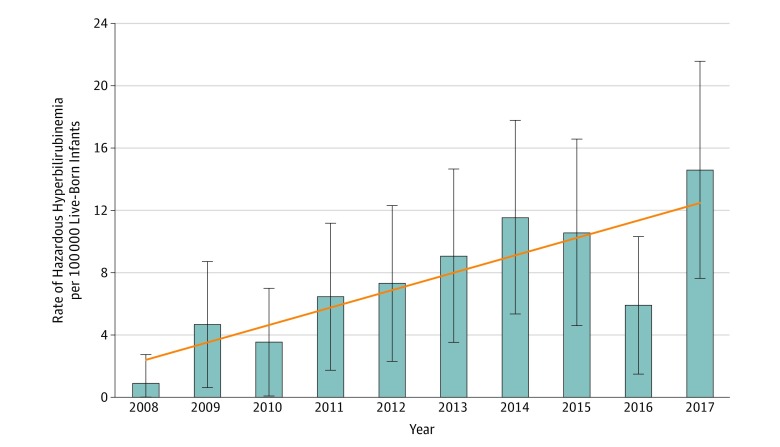
Results: Among 992 378 live-born infants (958 051 term births and 34 327 near-term births), 494 (320 boys; mean [SD] birth weight, 3505 [527] g) developed extreme hyperbilirubinemia (50 per 100 000 infants), 6.8 per 100 000 infants developed hazardous hyperbilirubinemia, and 1.3 per 100 000 infants developed kernicterus. Among 13 children developing kernicterus, brain injury was assessed as potentially avoidable for 11 children based on the presence of 1 or several of the following possible causes: untimely or lack of predischarge bilirubin screening (n = 6), misinterpretation of bilirubin values (n = 2), untimely or delayed initiation of treatment with intensive phototherapy (n = 1), untimely or no treatment with exchange transfusion (n = 6), or lack of repeated exchange transfusions despite indication (n = 1).
Conclusions and relevance: Hazardous hyperbilirubinemia in near-term or term newborns still occurs in Sweden and was associated with disabling brain damage in 13 per million births. For most of these cases, health care professional noncompliance with best practices was identified, suggesting that a substantial proportion of these cases might have been avoided.
Conflict of interest statement
Figures