

A Novel Gradient Echo Plural Contrast Imaging Method Detects Brain Tissue Abnormalities in Patients With TBI Without Evident Anatomical Changes on Clinical MRI: A Pilot Study
- PMID: 30901451
- PMCID: PMC6751359
- DOI: 10.1093/milmed/usy394
A Novel Gradient Echo Plural Contrast Imaging Method Detects Brain Tissue Abnormalities in Patients With TBI Without Evident Anatomical Changes on Clinical MRI: A Pilot Study
Abstract
Research objectives: It is widely accepted that mild traumatic brain injury (mTBI) causes injury to the white matter, but the extent of gray matter (GM) damage in mTBI is less clear.
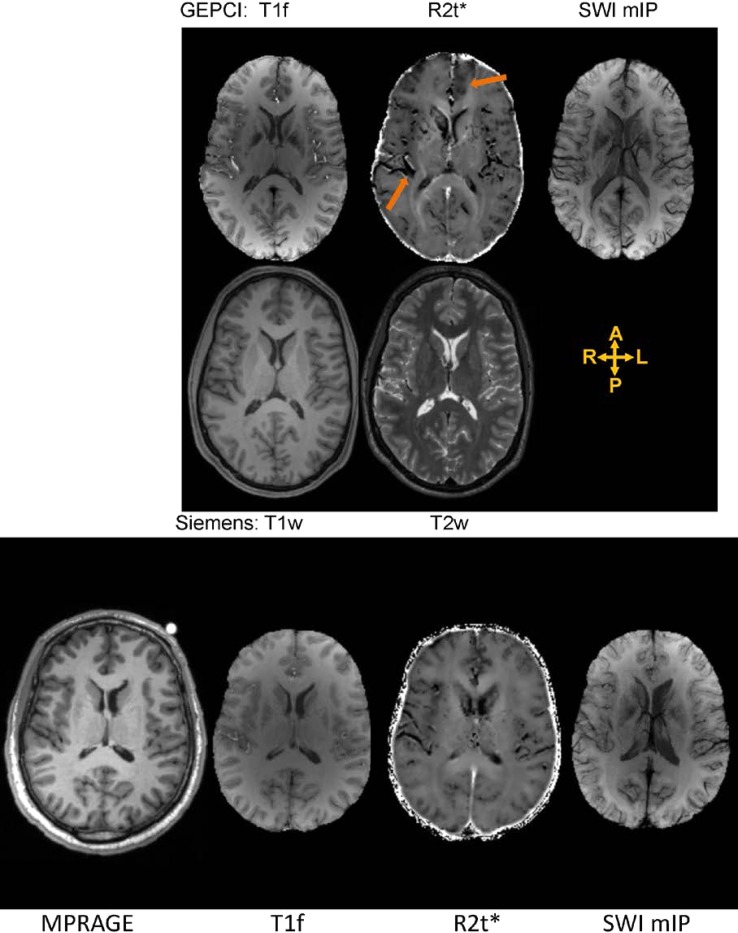
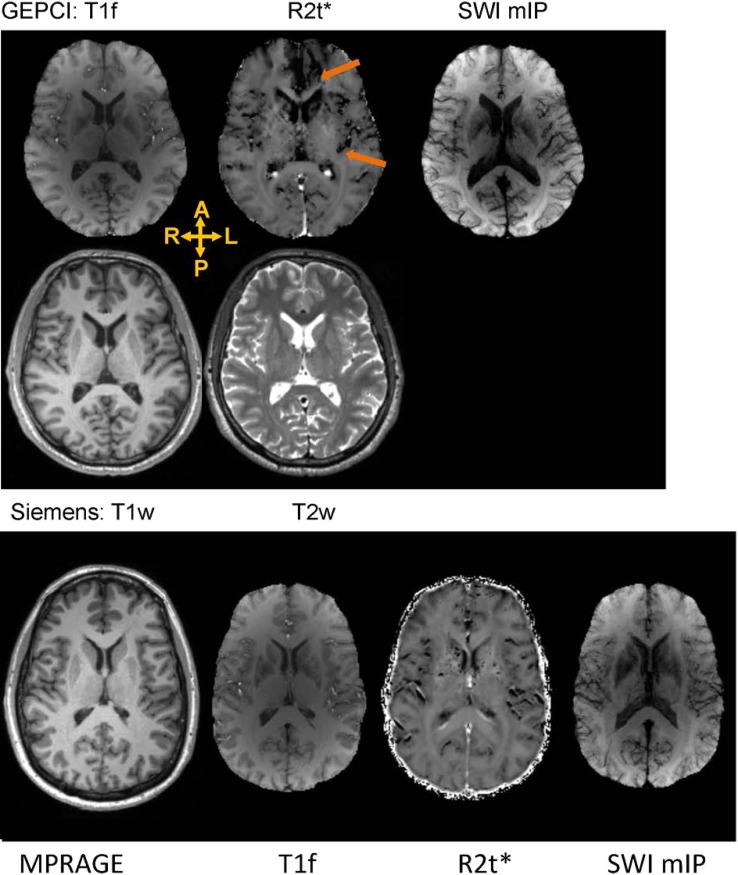
Methods: We tested 26 civilian healthy controls and 14 civilian adult subacute-chronic mTBI patients using quantitative features of MRI-based Gradient Echo Plural Contrast Imaging (GEPCI) technique. GEPCI data were reconstructed using previously developed algorithms allowing the separation of R2t*, a cellular-specific part of gradient echo MRI relaxation rate constant, from global R2* affected by BOLD effect and background gradients.
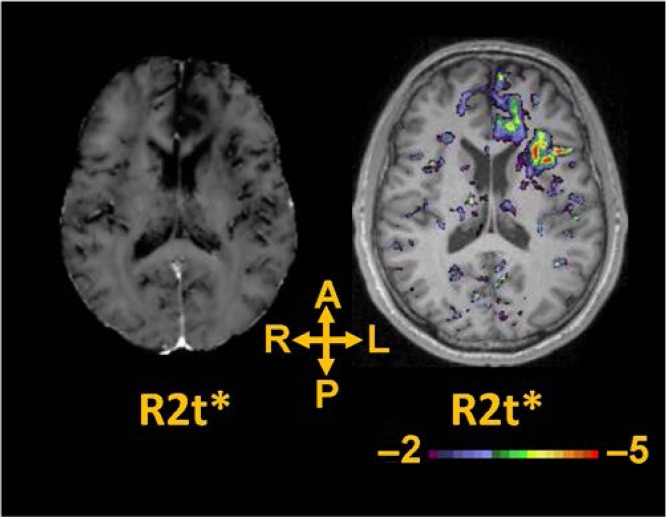
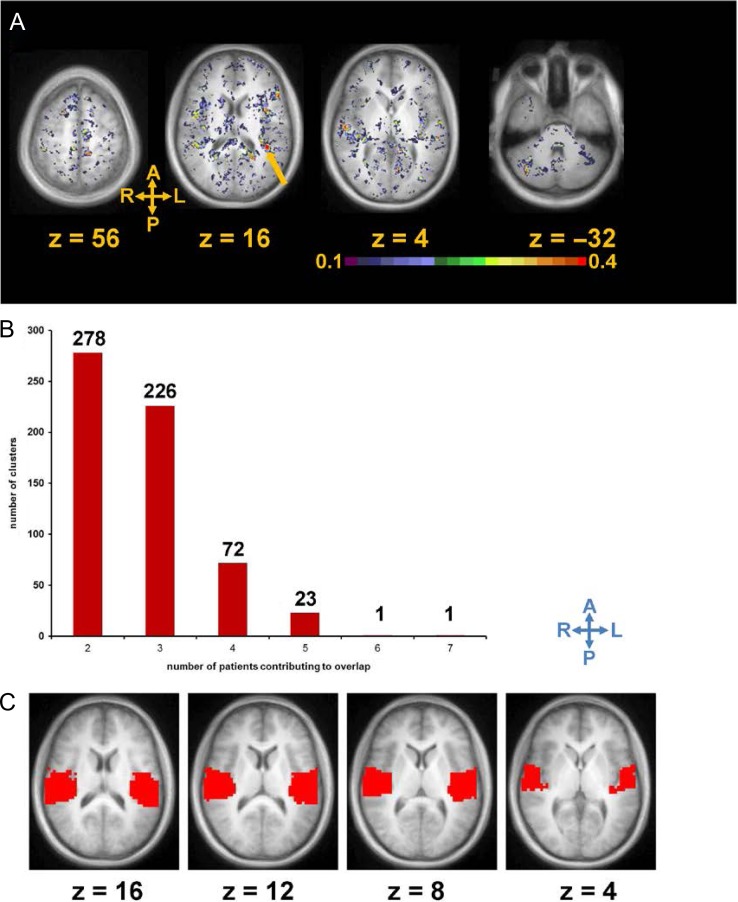
Results: Single-subject voxel-wise analysis (comparing each mTBI patient to the sample of 26 control subjects) revealed GM abnormalities that were not visible on standard MRI images (T1w and T2w). Analysis of spatial overlap for voxels with low R2t* revealed tissue abnormalities in multiple GM regions, especially in the frontal and temporal regions, that are frequently damaged after mTBI. The left posterior insula was the region with abnormalities found in the highest proportion (50%) of mTBI patients.
Conclusions: Our data suggest that GEPCI quantitative R2t* metric has potential to detect abnormalities in GM cellular integrity in individual TBI patients, including abnormalities that are not detectable by a standard clinical MRI.
Keywords: MRI; Traumatic Brain Injury; gray matter.
© Association of Military Surgeons of the United States 2019. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Faul M, Xu L, Wald MM, Coronado VG: Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths. Atlanta (GA), Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, 2010.
-
- Chen AJ, D’Esposito M: Traumatic brain injury: from bench to bedside [corrected] to society. Neuron 2010; 66(1): 11–4. - PubMed
-
- Crooks CY, Zumsteg JM, Bell KR: Traumatic brain injury: a review of practice management and recent advances. Phys Med Rehabil Clin N Am 2007; 18(4): 681–710. vi. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
