

Long-term control with chemoradiation of initially metastatic mixed adenoneuroendocrine carcinoma of the rectum: a case report
- PMID: 30902067
- PMCID: PMC6431024
- DOI: 10.1186/s13256-019-1995-x
Long-term control with chemoradiation of initially metastatic mixed adenoneuroendocrine carcinoma of the rectum: a case report
Abstract
Background: Mixed adenoneuroendocrine carcinomas are highly malignant tumors with both adenocarcinomatous and neuroendocrine components. They can originate in any organ but are more common in the rectum. Due to their rarity, current treatment recommendations for mixed adenoneuroendocrine carcinoma are based on limited data and follow general guidelines for the management of adenocarcinomas and neuroendocrine neoplasms. Uncertainty regarding the efficacy of the available local and systemic treatment strategies is a compounding issue. Even those patients with locally limited disease have a relatively short life expectancy. In this report, we describe a case of deep rectal mixed adenoneuroendocrine carcinoma with long survival after chemoradiation.
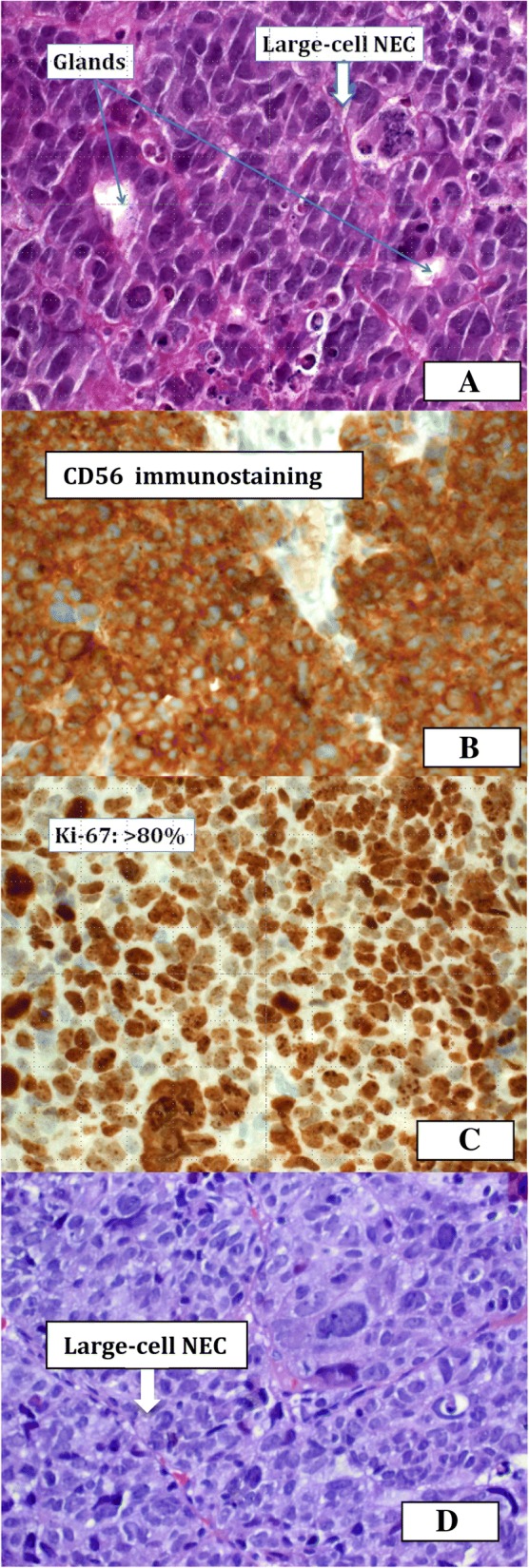
Case presentation: A 48-year-old Caucasian woman was diagnosed with a grade 3 rectal adenocarcinoma combined with a poorly differentiated large cell neuroendocrine carcinoma component and synchronous metastases (cT3cN1cM1) in both lobes of the liver in 2012. She received concomitant chemoradiotherapy followed by four additional cycles of cisplatin plus irinotecan. Initial treatment induced complete remission of the rectal tumor and liver metastases. Consequently, it was not necessary to surgically resect the primary tumor or any of the metastases. Three months after the end of treatment, one metastasis in the first segment of the liver showed regrowth, and stereotactic body radiotherapy of the metastasis and chemotherapy resulted in a clinical complete response. The patient has been recurrence-free for more than 5 years.
Conclusions: Extended long-term control of a poorly differentiated metastatic (stage IV) mixed adenoneuroendocrine carcinoma is rare. The multimodal first- and second-line regimens of radiotherapy and chemotherapy described in this case report represent a new therapeutic approach. Encouraged by the results in this case, we compiled a review of the literature on mixed adenoneuroendocrine carcinoma.
Keywords: Chemoradiation; MANEC; Rectum; SBRT.
Conflict of interest statement
Ethics approval and consent to participate
All procedures were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient agreed to receive all forms of therapy after appreciation and understanding of the facts, implication of the therapy, alternative treatment options and consequences of the treatment.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guideline in Oncology, Neuroendocrine Tumors, Version 3. 2017. https://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf. Accessed 19 Dec 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
