

LwPTL: a novel classification for upper airway collapse in sleep endoscopies
- PMID: 30902587
- PMCID: PMC9442889
- DOI: 10.1016/j.bjorl.2019.01.010
LwPTL: a novel classification for upper airway collapse in sleep endoscopies
Abstract
Introduction: There is no consensus on a single classification system for the obstructive findings in drug-induced sleep endoscopy. Previous classification systems have neglected to address the upper retropalatal obstruction, the segmental division of the lateral pharyngeal wall and the primary or secondary nature of laryngeal collapse.
Objective: To propose, illustrate and evaluate a more comprehensive and yet simple classification for drug-induced sleep endoscopy findings.
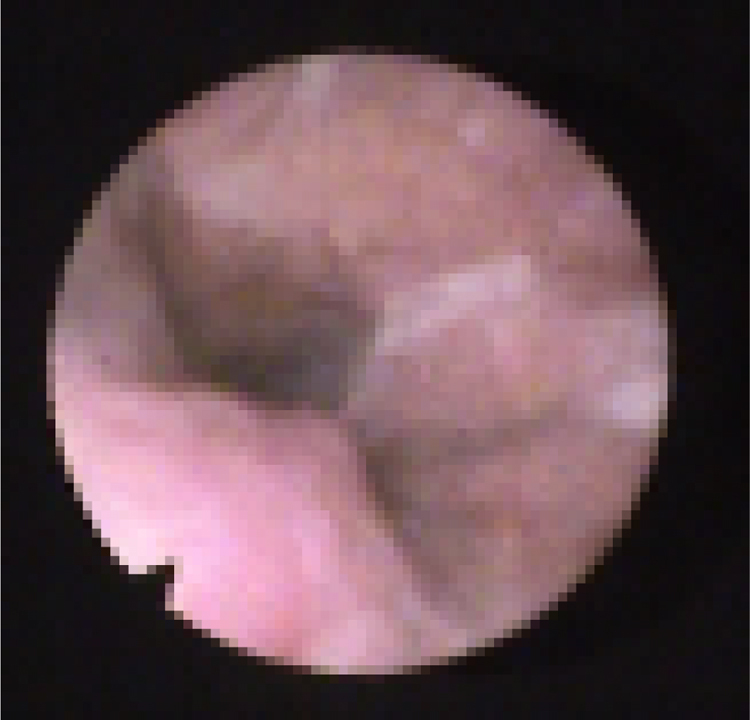
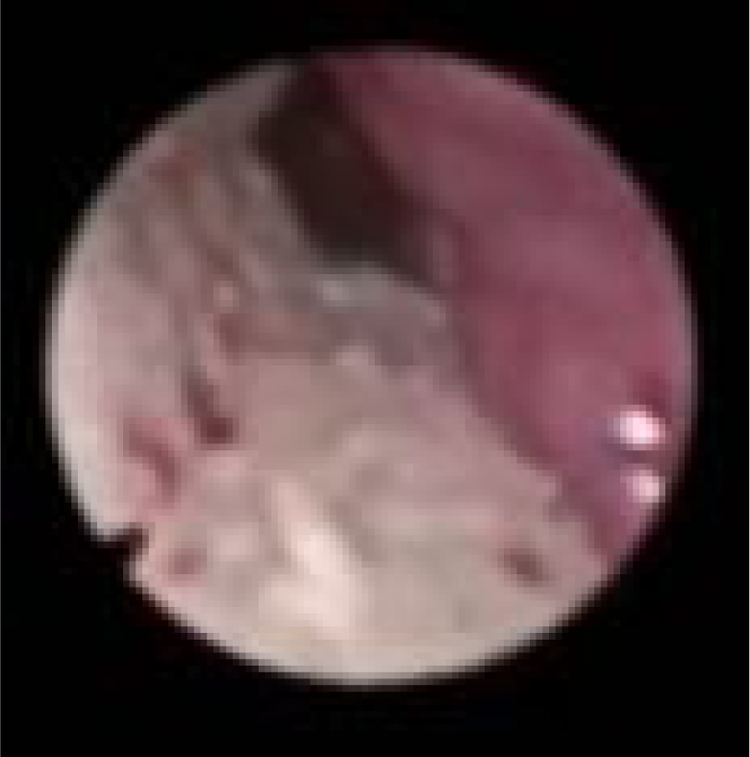
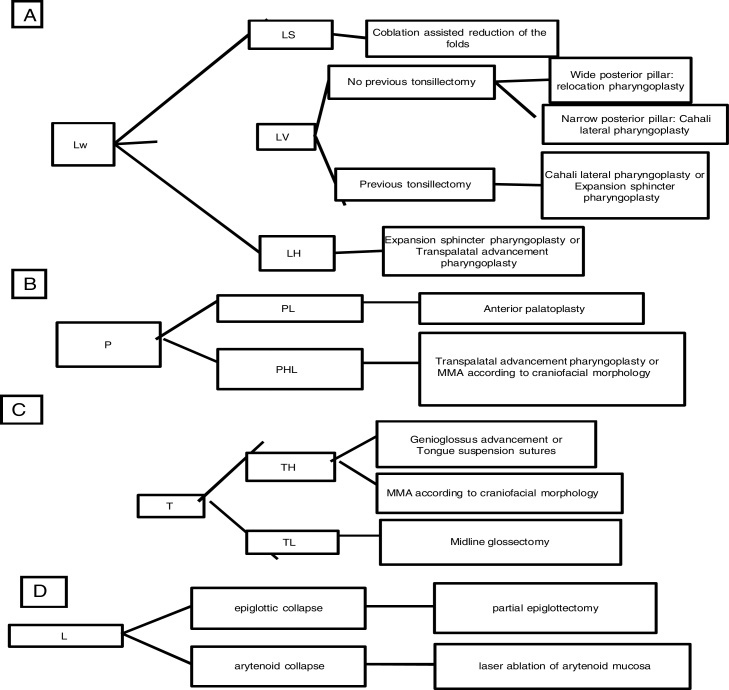
Methods: Cross sectional study in a tertiary sleep surgery unit. A total of 30 patients with obstructive sleep apnea underwent drug-induced sleep endoscopy according to a new classification system called LwPTL, and its findings were analyzed according to obstructive sleep apnea severity and body mass index. LwPTL incorporates the description of upper retropalatal collapse, distinguishes the lateral pharyngeal wall collapse into three levels and clarify when laryngeal collapses are primary or secondary.
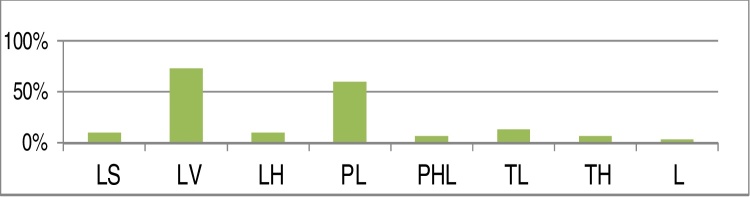
Results: 93.3% of the patients presented lateral pharyngeal wall collapse, usually at the level of the velum (73.3%). 80% presented multilevel collapse. Regarding the upper retropalatal region, LwPTL identified 10% of the cases presenting lateral salpingopharyngeal obstruction and 6.6% with high palatal collapse. 3.3% presented epiglottic collapse. Patients presenting lower levels of collapse, either from the lateral wall and/or tongue and/or larynx, represented 30% of the cases and had significantly more severe obstructive sleep apnea, without significant differences in body mass indexes.
Conclusion: LwPTL seems a simple and straightforward staging system for classifying drug-induced sleep endoscopy, distinguishing the important upper retopalatal obstruction and the primary and secondary laryngeal collapses, providing more information for appropriate treatment selection.
Introdução: Não há consenso sobre um sistema único de classificação para os achados obstrutivos da endoscopia do sono induzido por drogas. Os sistemas de classificação anteriores negligenciaram a abordagem da obstrução retropalatal alta, a divisão segmentar da parede lateral da faringe e a natureza primária ou secundária do colapso laríngeo.
Objetivo: Propor, ilustrar e avaliar uma classificação mais abrangente e simples para os achados da endoscopia do sono induzido por drogas.
Método: Estudo transversal em uma unidade terciária de cirurgia do sono. Foram submetidos à endoscopia do sono induzido por drogas 30 pacientes com apneia obstrutiva do sono, de acordo com um novo sistema de classificação denominado LwPTL, e seus achados foram analisados de acordo com a gravidade da apneia obstrutiva do sono e índice de massa corpórea .O LwPTL incorpora a descrição do colapso retropalatal alto, distingue o colapso da parede faríngea lateral em três níveis e esclarece quando os colapsos laríngeos são primários ou secundários.
Resultados: Apresentaram colapso da parede faríngea lateral 93,3% dos pacientes, geralmente no nível do palato mole (73,3%). Em 80% dos pacientes o colapso foi multinível. Em relação à região retropalatal alta, o LwPTL identificou 10% dos casos com obstrução salpingo-faríngea lateral e 6,6% com colapso alto do palato. Em 3,3% ocorreu colapso epiglótico. Pacientes com colapso em regiões baixas, tanto da parede lateral e/ou língua como e/ou laringe, representaram 30% dos casos e apresentaram apneia obstrutiva do sono significativamente mais grave, sem diferenças significantes no índice de massa corpórea.
Conclusão: O LwPTL parece um sistema de estadiamento simples e direto para classificar os achados da endoscopia do sono induzido por drogas, distingue a importante obstrução retropalatal alta e os colapsos laríngeos primários e secundários, fornece mais informações para uma seleção adequada do tratamento.
Keywords: Endoscopia; Endoscopy; Epiglote; Epiglottis; Faringe; Língua; Pharynx; Tongue.
Copyright © 2019 Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Published by Elsevier Editora Ltda. All rights reserved.
Figures









Similar articles
-
Association Between Soft Tissue Measures From Computed Tomography and Upper Airway Collapsibility on Drug-Induced Sleep Endoscopy.Otolaryngol Head Neck Surg. 2024 Aug;171(2):578-587. doi: 10.1002/ohn.772. Epub 2024 Apr 12. Otolaryngol Head Neck Surg. 2024. PMID: 38613204
-
[Research on the patterns of upper airway obstructive levels by drug-induced sleep endoscopy].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2014 Jan;49(1):58-61. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2014. PMID: 24680340 Chinese.
-
Efficacy of Upper Airway Stimulation on Collapse Patterns Observed during Drug-Induced Sedation Endoscopy.Otolaryngol Head Neck Surg. 2016 May;154(5):970-7. doi: 10.1177/0194599816636835. Epub 2016 Mar 15. Otolaryngol Head Neck Surg. 2016. PMID: 26980916
-
Drug-induced sleep endoscopy: techniques, interpretation and implications.Curr Opin Pulm Med. 2020 Nov;26(6):623-628. doi: 10.1097/MCP.0000000000000723. Curr Opin Pulm Med. 2020. PMID: 32890018 Review.
-
Obstructive sleep apnea and sedation in the endoscopy suite.Gastroenterol Nurs. 2006 Nov-Dec;29(6):456-63; quiz 464-5. doi: 10.1097/00001610-200611000-00004. Gastroenterol Nurs. 2006. PMID: 17273012 Review.
Cited by
-
Early-onset pharyngeal airway collapse in infants: a retrospective single-center study.BMC Pediatr. 2023 Nov 28;23(1):600. doi: 10.1186/s12887-023-04436-w. BMC Pediatr. 2023. PMID: 38017440 Free PMC article.
-
Transoral Drug-Induced Sleep Endoscopy: A Useful Complementary Tool in Sleep Surgery.Int Arch Otorhinolaryngol. 2025 Jan 10;29(1):1-8. doi: 10.1055/s-0044-1788768. eCollection 2025 Jan. Int Arch Otorhinolaryngol. 2025. PMID: 39801894 Free PMC article.
-
Role of transpalatal advancement pharyngoplasty in management of lateral pharyngeal wall collapse in OSA.Braz J Otorhinolaryngol. 2022 Nov-Dec;88 Suppl 1(Suppl 1):S82-S90. doi: 10.1016/j.bjorl.2021.04.009. Epub 2021 May 6. Braz J Otorhinolaryngol. 2022. PMID: 33994340 Free PMC article.
-
New non-invasive electrical stimulation devices for treatment of snoring and obstructive sleep apnoea: a systematic review.Sleep Breath. 2023 Mar;27(1):103-108. doi: 10.1007/s11325-022-02615-0. Epub 2022 Apr 23. Sleep Breath. 2023. PMID: 35460429
References
-
- Sutherland K., Cistulli P.A. Recent advances in obstructive sleep apnea pathophysiology and treatment. Sleep Biol Rhythms. 2015;13:26–40.
-
- Li H.Y., Lee L.A. Relocation pharyngoplasty for obstructive sleep apnea. Laryngoscope. 2009;119:2472–2477. - PubMed
-
- Vicini C., De Vito A., Benazzo M., Frassineti S., Campanini A., Frasconi P., et al. The Nose Oropharynx Hypopharynx and Larynx (NOHL) classification: a new system of diagnostic standardized examination for OSAHS patients. Eur Arch Otorhinolaryngol. 2012;269:1297–1300. - PubMed
-
- Hohenhorst W., Ravesloot M.J.L., Kezirian E.J., De Vries N. Drug-induced sleep endoscopy in adults with sleep-disordered breathing: technique and the VOTE Classification system. Oper Tech Otolaryngol Head Neck Surg. 2012;23:11–18.
-
- Croft C.B., Pringle M. Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci. 1991;16:504–509. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
