

The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study
- PMID: 30902669
- PMCID: PMC7646282
- DOI: 10.1016/S2215-0366(19)30048-3
The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study
Abstract
Background: Cannabis use is associated with increased risk of later psychotic disorder but whether it affects incidence of the disorder remains unclear. We aimed to identify patterns of cannabis use with the strongest effect on odds of psychotic disorder across Europe and explore whether differences in such patterns contribute to variations in the incidence rates of psychotic disorder.
Methods: We included patients aged 18-64 years who presented to psychiatric services in 11 sites across Europe and Brazil with first-episode psychosis and recruited controls representative of the local populations. We applied adjusted logistic regression models to the data to estimate which patterns of cannabis use carried the highest odds for psychotic disorder. Using Europe-wide and national data on the expected concentration of Δ9-tetrahydrocannabinol (THC) in the different types of cannabis available across the sites, we divided the types of cannabis used by participants into two categories: low potency (THC <10%) and high potency (THC ≥10%). Assuming causality, we calculated the population attributable fractions (PAFs) for the patterns of cannabis use associated with the highest odds of psychosis and the correlation between such patterns and the incidence rates for psychotic disorder across the study sites.
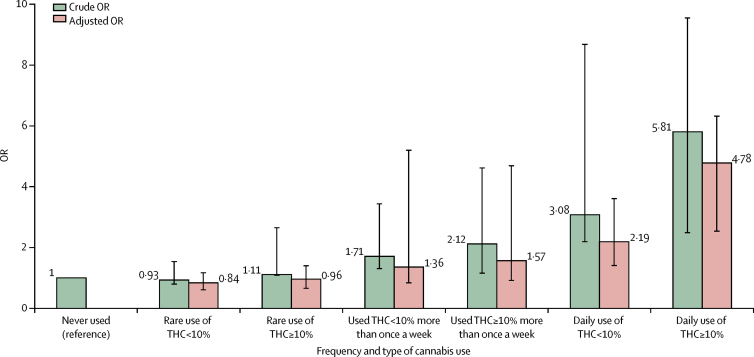
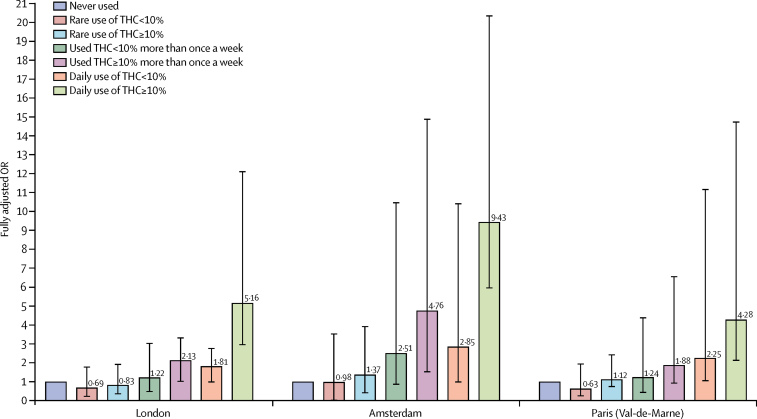
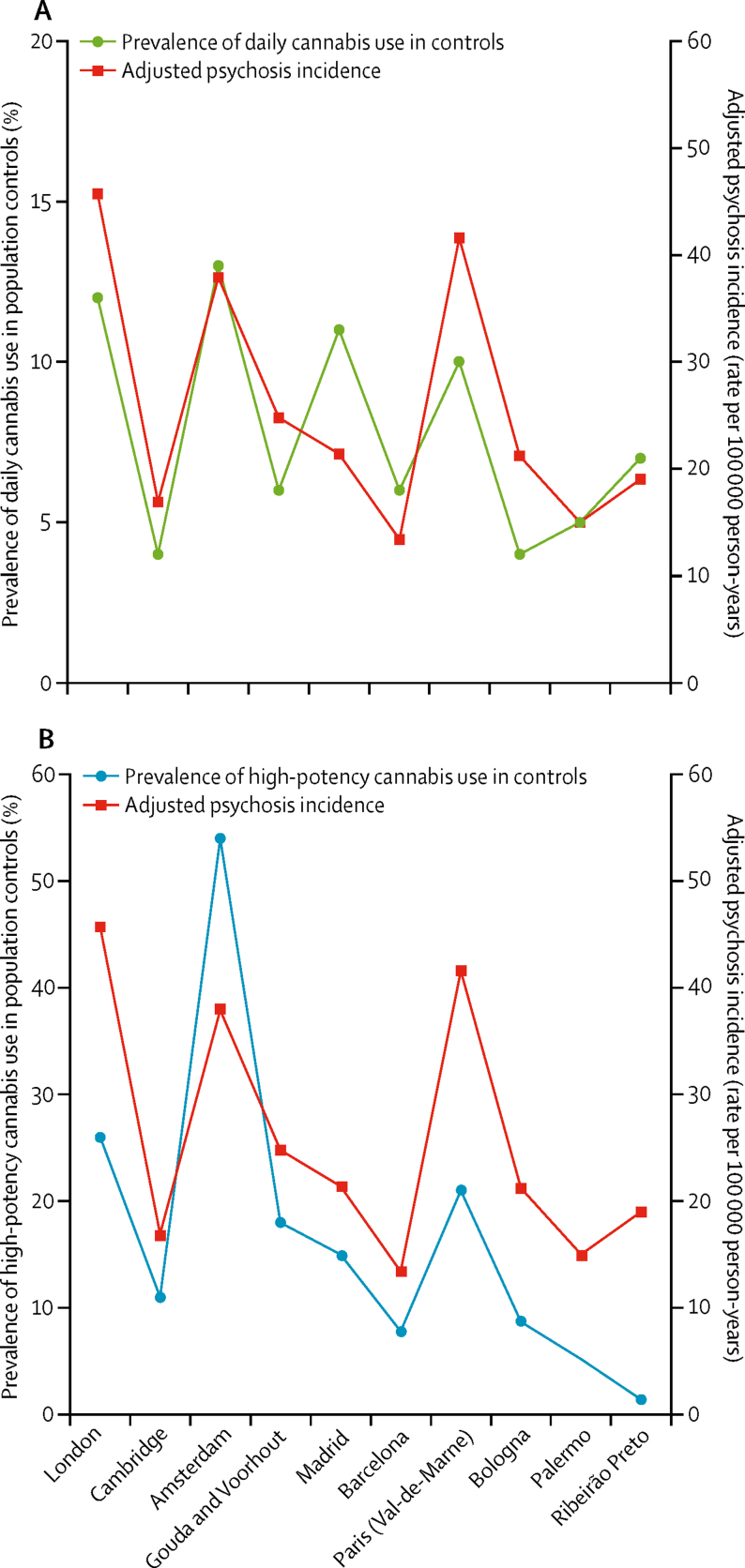
Findings: Between May 1, 2010, and April 1, 2015, we obtained data from 901 patients with first-episode psychosis across 11 sites and 1237 population controls from those same sites. Daily cannabis use was associated with increased odds of psychotic disorder compared with never users (adjusted odds ratio [OR] 3·2, 95% CI 2·2-4·1), increasing to nearly five-times increased odds for daily use of high-potency types of cannabis (4·8, 2·5-6·3). The PAFs calculated indicated that if high-potency cannabis were no longer available, 12·2% (95% CI 3·0-16·1) of cases of first-episode psychosis could be prevented across the 11 sites, rising to 30·3% (15·2-40·0) in London and 50·3% (27·4-66·0) in Amsterdam. The adjusted incident rates for psychotic disorder were positively correlated with the prevalence in controls across the 11 sites of use of high-potency cannabis (r = 0·7; p=0·0286) and daily use (r = 0·8; p=0·0109).
Interpretation: Differences in frequency of daily cannabis use and in use of high-potency cannabis contributed to the striking variation in the incidence of psychotic disorder across the 11 studied sites. Given the increasing availability of high-potency cannabis, this has important implications for public health.
Funding source: Medical Research Council, the European Community's Seventh Framework Program grant, São Paulo Research Foundation, National Institute for Health Research (NIHR) Biomedical Research Centre (BRC) at South London and Maudsley NHS Foundation Trust and King's College London and the NIHR BRC at University College London, Wellcome Trust.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Cannabis and psychosis: triangulating the evidence.Lancet Psychiatry. 2019 May;6(5):364-365. doi: 10.1016/S2215-0366(19)30086-0. Epub 2019 Mar 19. Lancet Psychiatry. 2019. PMID: 30902668 No abstract available.
-
High-potency cannabis and incident psychosis: correcting the causal assumption.Lancet Psychiatry. 2019 Jun;6(6):464-465. doi: 10.1016/S2215-0366(19)30130-0. Lancet Psychiatry. 2019. PMID: 31122471 No abstract available.
-
High-potency cannabis and incident psychosis: correcting the causal assumption.Lancet Psychiatry. 2019 Jun;6(6):464. doi: 10.1016/S2215-0366(19)30174-9. Lancet Psychiatry. 2019. PMID: 31122472 No abstract available.
-
High-potency cannabis and incident psychosis: correcting the causal assumption.Lancet Psychiatry. 2019 Jun;6(6):465-466. doi: 10.1016/S2215-0366(19)30175-0. Lancet Psychiatry. 2019. PMID: 31122473 No abstract available.
-
High-potency cannabis and incident psychosis: correcting the causal assumption.Lancet Psychiatry. 2019 Jun;6(6):e14. doi: 10.1016/S2215-0366(19)30178-6. Lancet Psychiatry. 2019. PMID: 31122483 No abstract available.
References
-
- Hall W, Lynskey M. Evaluating the public health impacts of legalizing recreational cannabis use in the United States. Addiction. 2016;111:1764–1773. - PubMed
-
- Gage SH, Hickman M, Zammit S. Association between cannabis and psychosis: epidemiologic evidence. Biol Psychiatry. 2016;79:549–556. - PubMed
-
- Mustonen A, Niemelä S, Nordström T. Adolescent cannabis use, baseline prodromal symptoms and the risk of psychosis. Br J Psychiatry. 2018;212:227–233. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
