

Etiology of 305 cases of refractory hematospermia and therapeutic options by emerging endoscopic technology
- PMID: 30903016
- PMCID: PMC6430789
- DOI: 10.1038/s41598-019-41123-2
Etiology of 305 cases of refractory hematospermia and therapeutic options by emerging endoscopic technology
Abstract
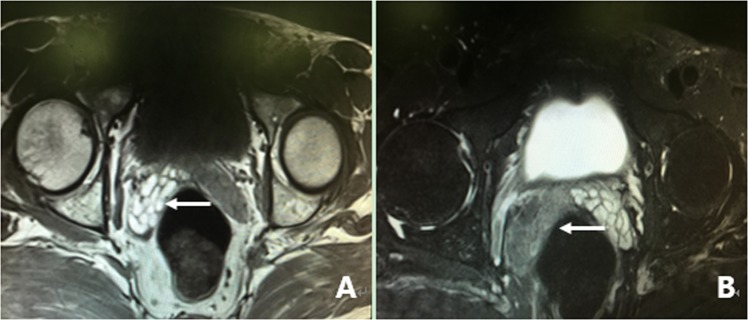
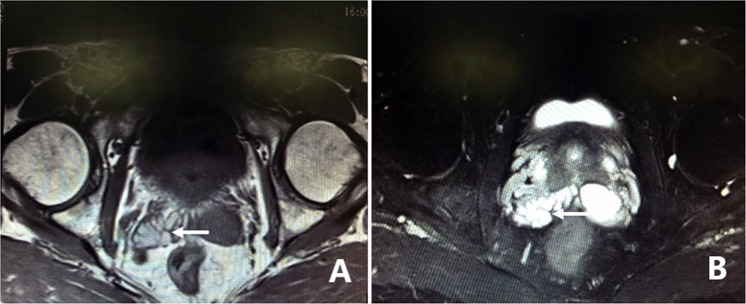
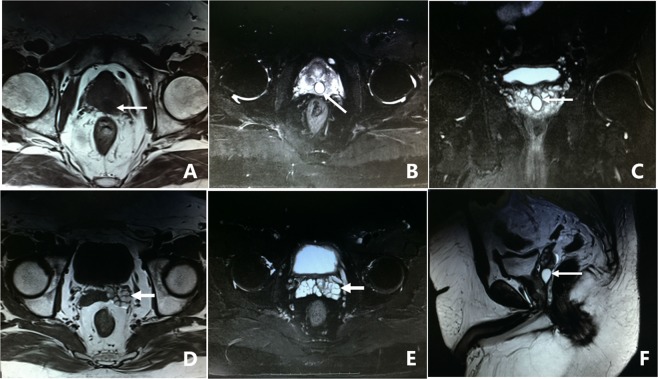
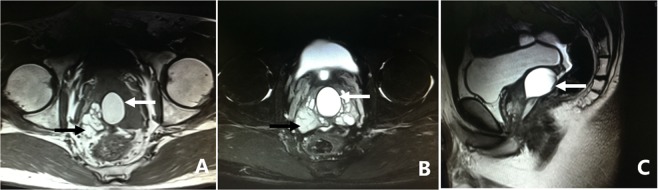
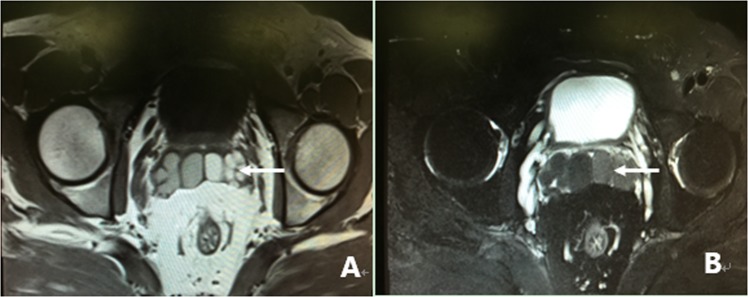
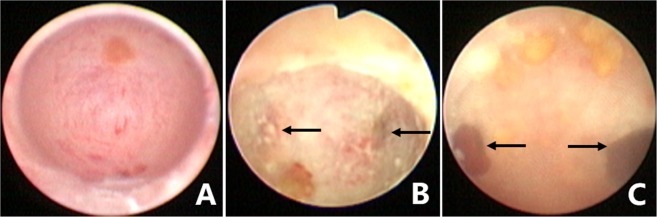
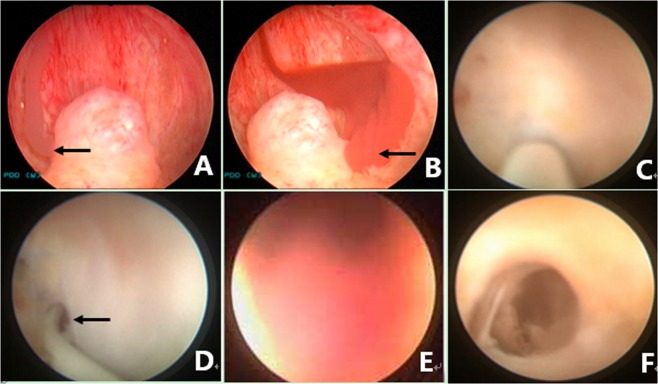
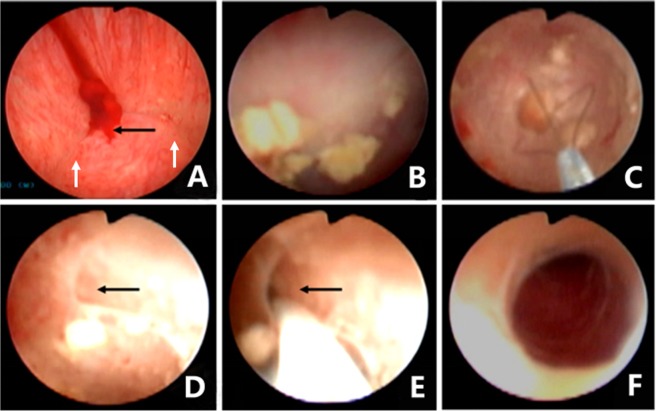
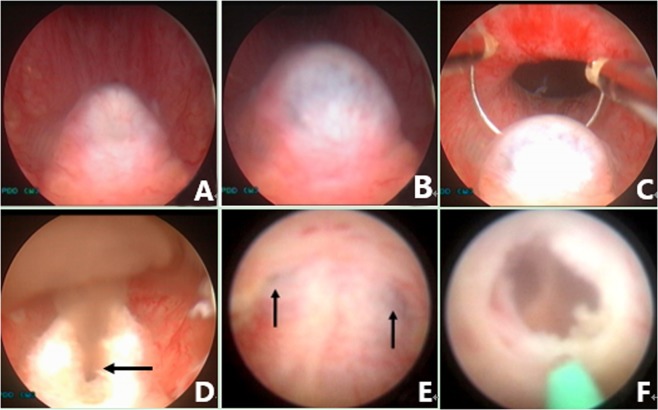
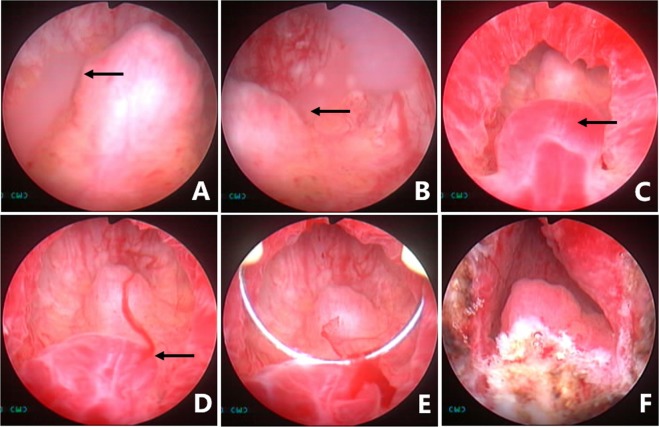
To investigate the surgical outcomes of vesiculoscopy on refractory hematospermia and ejaculatory duct obstruction (EDO), the clinical data (including pelvic magnetic resonance imaging (MRI) examinations and the long-term effects of endoscopic treatment) from 305 patients were analyzed. Four main etiologic groups were found on MRI. We found that 62.0% (189/305) of patients showed abnormal signal intensity in MRI investigations in the seminal vesicle (SV) area. Cystic lesions were observed in 36.7% (112/305) of the patients. The third sign was dilatation or enlargement of unilateral or bilateral SV, which were observed in 32.1% (98/305) of the patients. The fourth sign was stone formation in SV or in an adjacent cyst, which was present in 8.5% (26/305) of the patients. The transurethral endoscopy or seminal vesiculoscopy and the related procedures, including fenestration in prostatic utricle (PU), irrigation, lithotripsy, stone removal, biopsy, electroexcision, fulguration, or transurethral resection/incision of the ejaculatory duct (TURED/TUIED), chosen according to the different situations of individual patients were successfully performed in 296 patients. Fenestrations in PU+ seminal vesiculoscopy were performed in 66.6% (197/296) of cases. Seminal vesiculoscopy via the pathological opening in PU was performed in 10.8% (32/296) of cases. TURED/TUIED + seminal vesiculoscopy was performed in 12.8% (38/296) of cases, and seminal vesiculoscopy by the natural orifices of the ejaculatory duct (ED) was performed in 2.4% (7/296) of cases. Electroexcision and fulguration to the abnormal blood vessels or cavernous hemangioma at posterior urethra were performed in 7.4% (22/296) of cases. Two hundred and seventy-one patients were followed up for 6-72 months. The hematospermia of all the patients disappeared within 2-6 weeks, and 93.0% of the patients showed no further hematospermia during follow-up. No obvious postoperative complications were observed. The transurethral seminal vesiculoscopy technique and related procedures are safe and effective approaches for refractory hematospermia and EDO.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Polito M, et al. Hematospermia: diagnosis and treatment. Arch Ital Urol Androl. 2006;78:82–85. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
