

Ten Years of Robotripping: Evidence of Tolerance to Dextromethorphan Hydrobromide in a Long-Term User
- PMID: 30903576
- PMCID: PMC6597748
- DOI: 10.1007/s13181-019-00706-1
Ten Years of Robotripping: Evidence of Tolerance to Dextromethorphan Hydrobromide in a Long-Term User
Abstract
Introduction: Dextromethorphan hydrobromide is widely available as an over-the-counter cough suppressant. A semi-synthetic opioid displaying N-methyl-D-aspartate receptor antagonism, it is commonly abused for recreational purposes. Spuriously elevated serum chloride concentrations are a well-described phenomenon in the setting of dextromethorphan hydrobromide toxicity, but evidence to suggest the development of tolerance is limited to case reports.
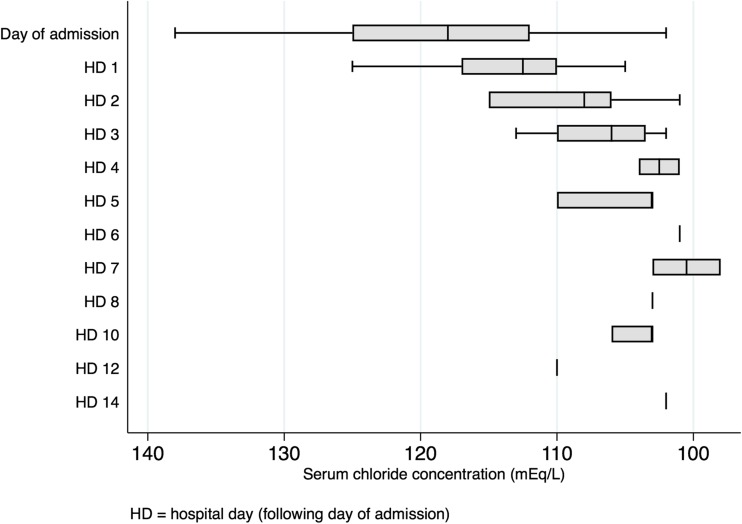
Case: A 32-year-old male known to chronically ingest dextromethorphan hydrobromide for recreational purposes presented to regional hospitals on 179 occasions over 110 months and was treated for dextromethorphan toxicity on 163/174 (93.7%) of these visits. He reported a subjective need to increase his dosing over time to achieve the same degree of intoxication. Measured serum chloride over this period (n = 217) ranged from 98 to 138 mEq/L (median 115 mEq/L, IQR 110-123 mEq/L). Measured concentrations over the 110-month period progressively rose, with a fitted plot of 111.15 + 0.00232x describing the rise in measured chloride. Though not formally assessed, anion gaps tended to become progressively more negative over the observed period.
Discussion: We report a patient with persistent dextromethorphan hydrobromide abuse at escalating doses whose mean serum chloride concentration increased, on average, by 0.00232 mEq/L every day over a 110-month period. This case demonstrates progressive spurious hyperchloremia secondary to bromide interference in hospital-based chloride assays, supporting the patient's reported need to dose escalate to the same desired effect. Although this artefactual laboratory finding is a well-documented result of bromide ingestion, it may be useful in identifying patterns of dextromethorphan hydrobromide use that suggest tolerance.
Keywords: Bromism; Dextromethorphan; Hyperchloremia; Robotripping; Tolerance.
Conflict of interest statement
None.
Figures



Similar articles
-
Spurious hyperchloremia and decreased anion gap in a patient with dextromethorphan bromide.Am J Nephrol. 1992;12(4):268-70. doi: 10.1159/000168457. Am J Nephrol. 1992. PMID: 1481876
-
Bromide intoxication by the combination of bromide-containing over-the-counter drug and dextromethorphan hydrobromide.Hum Exp Toxicol. 2003 Aug;22(8):459-61. doi: 10.1191/0960327103ht380cr. Hum Exp Toxicol. 2003. PMID: 12948087
-
Bromism: An overlooked and elusive toxidrome from chronic dextromethorphan abuse.Am J Emerg Med. 2020 Aug;38(8):1696.e1. doi: 10.1016/j.ajem.2019.158491. Epub 2019 Nov 15. Am J Emerg Med. 2020. PMID: 31864868
-
Recreational use of dextromethorphan, "Robotripping"-A brief review.Am J Addict. 2016 Aug;25(5):374-7. doi: 10.1111/ajad.12389. Epub 2016 Jun 11. Am J Addict. 2016. PMID: 27288091 Review.
-
Abuse of over-the-counter dextromethorphan by teenagers.South Med J. 1993 Oct;86(10):1151-3. doi: 10.1097/00007611-199310000-00014. South Med J. 1993. PMID: 8211334 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
