

Effect of Additional Oral Semaglutide vs Sitagliptin on Glycated Hemoglobin in Adults With Type 2 Diabetes Uncontrolled With Metformin Alone or With Sulfonylurea: The PIONEER 3 Randomized Clinical Trial
- PMID: 30903796
- PMCID: PMC6484814
- DOI: 10.1001/jama.2019.2942
Effect of Additional Oral Semaglutide vs Sitagliptin on Glycated Hemoglobin in Adults With Type 2 Diabetes Uncontrolled With Metformin Alone or With Sulfonylurea: The PIONEER 3 Randomized Clinical Trial
Abstract
Importance: Phase 3 trials have not compared oral semaglutide, a glucagon-like peptide 1 receptor agonist, with other classes of glucose-lowering therapy.
Objective: To compare efficacy and assess long-term adverse event profiles of once-daily oral semaglutide vs sitagliptin, 100 mg added on to metformin with or without sulfonylurea, in patients with type 2 diabetes.
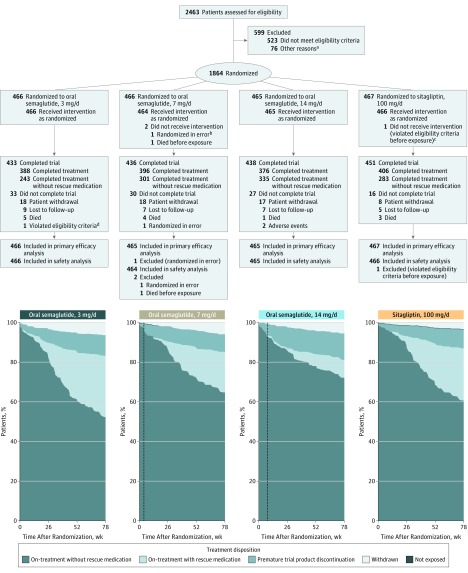
Design, setting, and participants: Randomized, double-blind, double-dummy, parallel-group, phase 3a trial conducted at 206 sites in 14 countries over 78 weeks from February 2016 to March 2018. Of 2463 patients screened, 1864 adults with type 2 diabetes uncontrolled with metformin with or without sulfonylurea were randomized.
Interventions: Patients were randomized to receive once-daily oral semaglutide, 3 mg (n = 466), 7 mg (n = 466), or 14 mg (n = 465), or sitagliptin, 100 mg (n = 467). Semaglutide was initiated at 3 mg/d and escalated every 4 weeks, first to 7 mg/d then to 14 mg/d, until the randomized dosage was achieved.
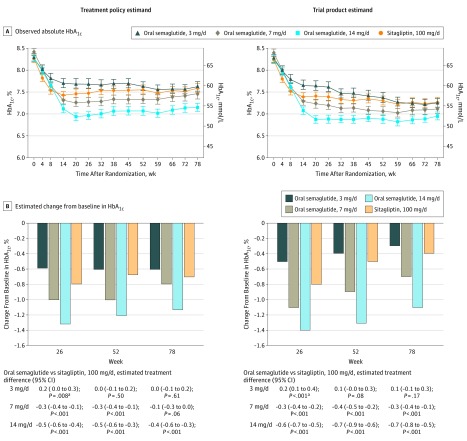
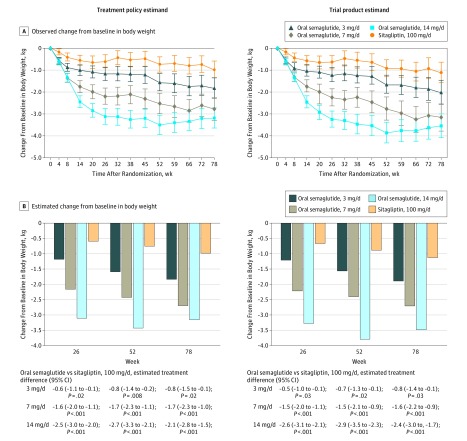
Main outcomes and measures: The primary end point was change in glycated hemoglobin (HbA1c), and the key secondary end point was change in body weight, both from baseline to week 26. Both were assessed at weeks 52 and 78 as additional secondary end points. End points were tested for noninferiority with respect to HbA1c (noninferiority margin, 0.3%) prior to testing for superiority of HbA1c and body weight.
Results: Among 1864 patients randomized (mean age, 58 [SD, 10] years; mean baseline HbA1c, 8.3% [SD, 0.9%]; mean body mass index, 32.5 [SD, 6.4]; n=879 [47.2%] women), 1758 (94.3%) completed the trial and 298 prematurely discontinued treatment (16.7% for semaglutide, 3 mg/d; 15.0% for semaglutide, 7 mg/d; 19.1% for semaglutide, 14 mg/d; and 13.1% for sitagliptin). Semaglutide, 7 and 14 mg/d, compared with sitagliptin, significantly reduced HbA1c (differences, -0.3% [95% CI, -0.4% to -0.1%] and -0.5% [95% CI, -0.6% to -0.4%], respectively; P < .001 for both) and body weight (differences, -1.6 kg [95% CI, -2.0 to -1.1 kg] and -2.5 kg [95% CI, -3.0 to -2.0 kg], respectively; P < .001 for both) from baseline to week 26. Noninferiority of semaglutide, 3 mg/d, with respect to HbA1c was not demonstrated. Week 78 reductions in both end points were statistically significantly greater with semaglutide, 14 mg/d, vs sitagliptin.
Conclusions and relevance: Among adults with type 2 diabetes uncontrolled with metformin with or without sulfonylurea, oral semaglutide, 7 mg/d and 14 mg/d, compared with sitagliptin, resulted in significantly greater reductions in HbA1c over 26 weeks, but there was no significant benefit with the 3-mg/d dosage. Further research is needed to assess effectiveness in a clinical setting.
Trial registration: ClinicalTrials.gov Identifier: NCT02607865.
Conflict of interest statement
Figures
Comment in
-
The Future of the GLP-1 Receptor Agonists.JAMA. 2019 Apr 16;321(15):1457-1458. doi: 10.1001/jama.2019.2941. JAMA. 2019. PMID: 30903797 No abstract available.
-
In uncontrolled type 2 diabetes, adjunctive semaglutide reduced HbA1c and body weight vs sitagliptin.Ann Intern Med. 2019 Aug 20;171(4):JC16. doi: 10.7326/ACPJ201908200-016. Ann Intern Med. 2019. PMID: 31426059 No abstract available.
References
-
- Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018: a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669-2701. doi: 10.2337/dci18-0033 - DOI - PMC - PubMed
-
- Tran S, Retnakaran R, Zinman B, Kramer CK. Efficacy of glucagon-like peptide-1 receptor agonists compared to dipeptidyl peptidase-4 inhibitors for the management of type 2 diabetes: a meta-analysis of randomized clinical trials. Diabetes Obes Metab. 2018;20(suppl 1):68-76. doi: 10.1111/dom.13137 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
