

When and How to Operate Fragility Fractures of the Pelvis?
- PMID: 30905993
- PMCID: PMC6394185
- DOI: 10.4103/ortho.IJOrtho_631_17
When and How to Operate Fragility Fractures of the Pelvis?
Abstract
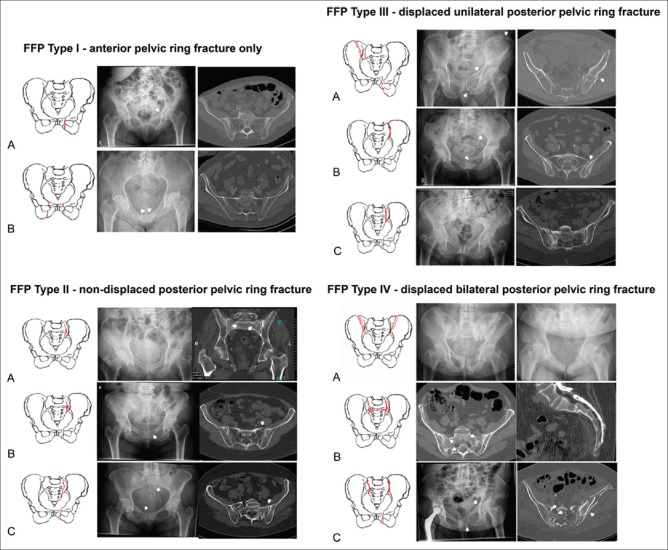
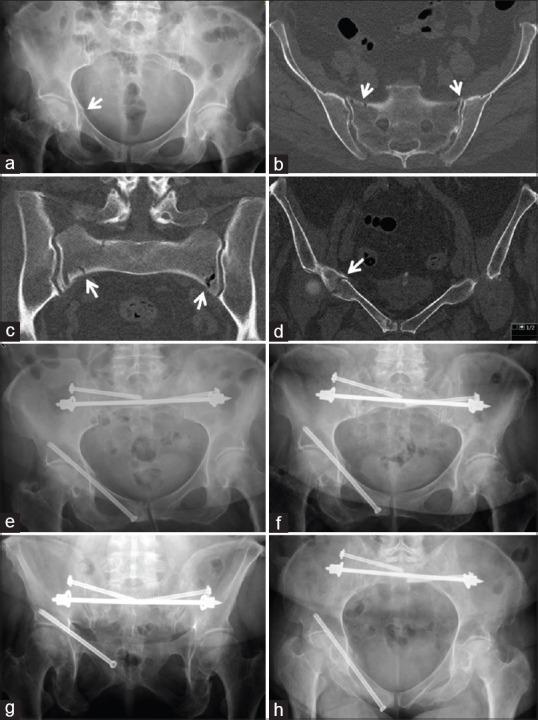
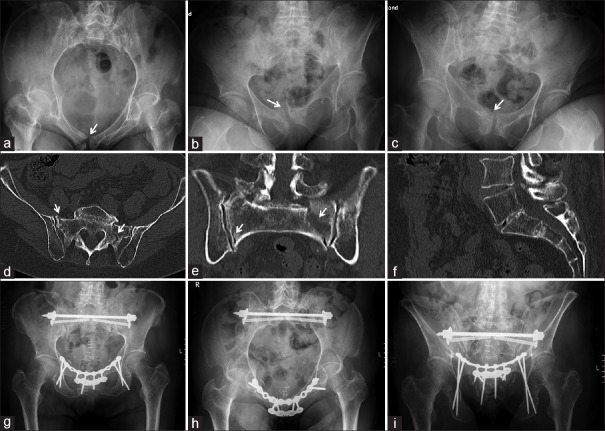
Fragility fractures of the pelvis (FFP) are an entity with an increasing frequency. The characteristics of these fractures are different from pelvic ring fractures in younger adults. There is a low energy instead of a high energy trauma mechanism. Due to a specific and consistent decrease of bone mineral density, typical fractures in the anterior and posterior pelvic ring occur. Bilateral sacral ala fractures are frequent. A new classification system distinguishes between four categories with increasing loss of stability. The subtypes represent different localizations of fractures. The primary goal of treatment is restoring mobility and independency. Depending on the amount of instability, conservative or surgical treatment is recommended. The operative technique should be as less invasive as possible. When the broken posterior pelvic ring is fixed operatively, a surgical fixation of the anterior pelvic ring should be considered as well. FFP Type I can be treated conservatively. In many cases, FFP Type II can also be treated conservatively. When conservative treatment fails, percutaneous fixation is performed. FFP Type III and FFP Type IV are treated operatively. The choice of the operation technique is depending on the localization of the fracture. Iliosacral screw osteosynthesis, transsacral bar osteosynthesis, transiliac internal fixation, and iliolumbar fixation are alternatives for stabilization of the posterior pelvic ring. Plate osteosynthesis, retrograde transpubic screw, and anterior internal fixation are alternatives for stabilization of the anterior pelvic ring. Postoperatively, early mobilization, with weight bearing as tolerated, is started. Simultaneously, bone metabolism is also analyzed and its defects compensated. Medical comorbidities should be identified and treated with the help of a multidisciplinary team.
Keywords: Characteristics; classification; fragility fractures pelvis; geriatric comanagement; minimally invasive; surgical fixation.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, et al. Osteoporosis in the European union: Medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA) Arch Osteoporos. 2013;8:136. - PMC - PubMed
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726–33. - PubMed
-
- Watts NB. The fracture risk assessment tool (FRAX®): Applications in clinical practice. J Womens Health (Larchmt) 2011;20:525–31. - PubMed
-
- Sullivan MP, Baldwin KD, Donegan DJ, Mehta S, Ahn J. Geriatric fractures about the hip: Divergent patterns in the proximal femur, acetabulum, and pelvis. Orthopedics. 2014;37:151–7. - PubMed
LinkOut - more resources
Full Text Sources