

Management of traumatic esophageal injuries
- PMID: 30906582
- PMCID: PMC6389559
- DOI: 10.21037/jtd.2018.10.86
Management of traumatic esophageal injuries
Abstract
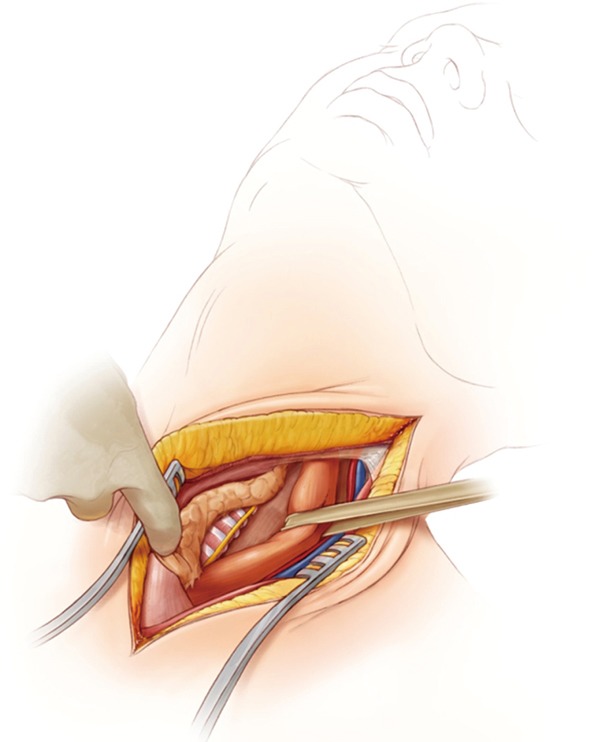
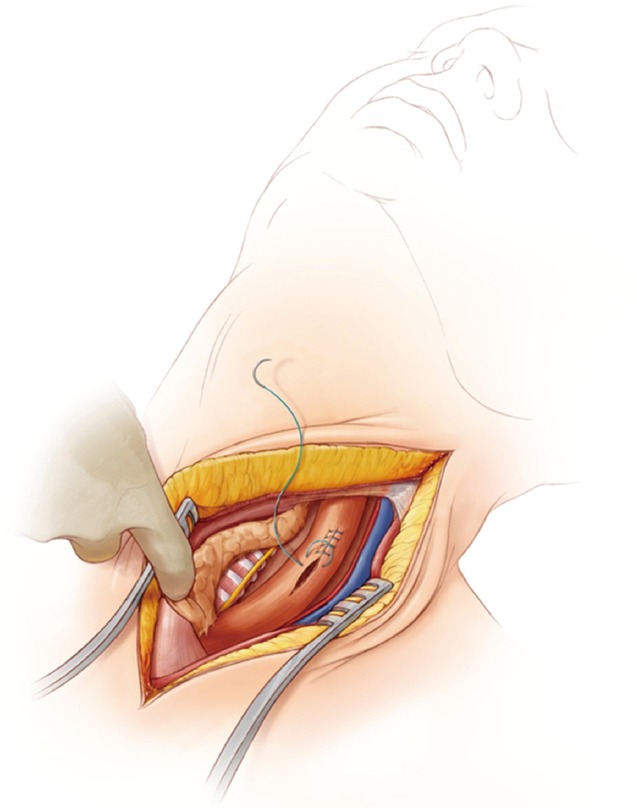
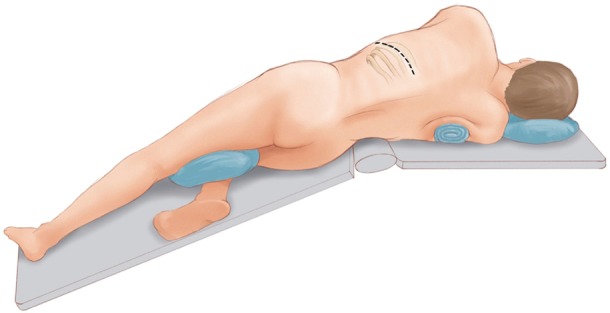
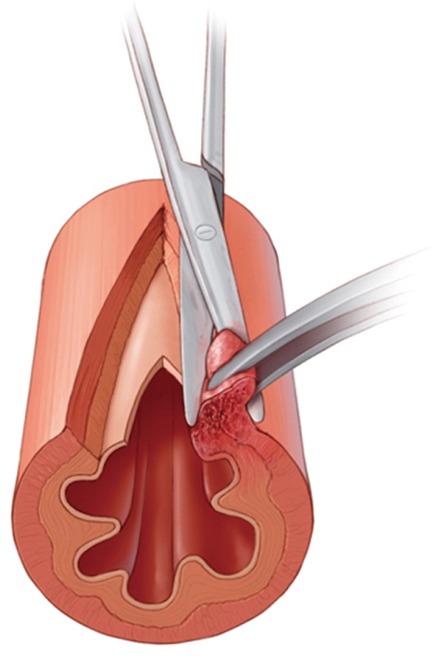
Traumatic esophageal perforations are rare but difficult to treat injuries. We review the principles of work-up, anatomy and treatment of cervical, thoracic and abdominal traumatic esophageal perforations. Management is dictated by location of the perforation and any concurrent injuries. The majority of cases are amenable to primary repair with flap re-enforcement. Other principles include adequate drainage around the repair, decompression of the esophagus and stomach (via nasogastric tube or gastrostomy tube) and distal enteral nutrition (feeding jejunostomy).
Keywords: Esophagus; esophageal leak; esophageal repair; esophageal trauma; perforations.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures







References
Publication types
LinkOut - more resources
Full Text Sources