

Recalibration and External Validation of the Risk Analysis Index: A Surgical Frailty Assessment Tool
- PMID: 30907757
- PMCID: PMC8785437
- DOI: 10.1097/SLA.0000000000003276
Recalibration and External Validation of the Risk Analysis Index: A Surgical Frailty Assessment Tool
Abstract
Objective and background: The Risk Analysis Index (RAI) predicts 30-, 180-, and 365-day mortality based on variables constitutive of frailty. Initially validated, in a single-center Veteran hospital, we sought to improve model performance by recalibrating the RAI in a large, veteran surgical registry, and to externally validate it in both a national surgical registry and a cohort of surgical patients for whom RAI was measured prospectively before surgery.
Methods: The RAI was recalibrated among development and confirmation samples within the Veterans Affairs Surgical Quality Improvement Program (VASQIP; 2010-2014; N = 480,731) including major, elective noncardiac surgery patients to create the revised RAI (RAI-rev), comparing discrimination and calibration. The model was tested externally in the American College of Surgeons National Surgical Quality Improvement Program dataset (NSQIP; 2005-2014; N = 1,391,785), and in a prospectively collected cohort from the Nebraska Western Iowa Health Care System VA (NWIHCS; N = 6,856).
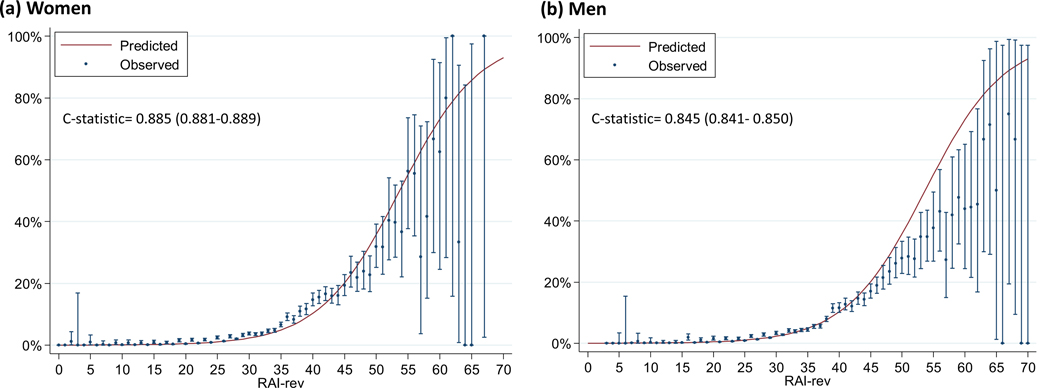
Results: Recalibrating the RAI significantly improved discrimination for 30-day [c = 0.84-0.86], 180-day [c = 0.81-0.84], and 365-day mortality [c = 0.78-0.82] (P < 0.001 for all) in VASQIP. The RAI-rev also had markedly better calibration (median absolute difference between observed and predicted 180-day mortality: decreased from 8.45% to 1.23%). RAI-rev was highly predictive of 30-day mortality (c = 0.87) in external validation with excellent calibration (median absolute difference between observed and predicted 30-day mortality: 0.6%). The discrimination was highly robust in men (c = 0.85) and women (c = 0.89). Discrimination also improved in the prospectively measured cohort from NWIHCS for 180-day mortality [c = 0.77 to 0.80] (P < 0.001).
Conclusions: The RAI-rev has improved discrimination and calibration as a frailty-screening tool in surgical patients. It has robust external validity in men and women across a wide range of surgical settings and available for immediate implementation for risk assessment and counseling in preoperative patients.
Conflict of interest statement
Conflict of Interest Disclosures:. Dr. Johanning holds intellectual property on frailty through FutureAssure, LLC. No other disclosures are reported.
Figures

References
-
- Kwok AC, Semel ME, Lipsitz SR, et al. The intensity and variation of surgical care at the end of life: a retrospective cohort study. Lancet. 2011;378(9800):1408–1413. - PubMed
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in Older Adults: Evidence for a Phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2001;56(3):M146–M157. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
