

Functional Outcome of Intravenous Thrombolysis in Patients With Lacunar Infarcts in the WAKE-UP Trial
- PMID: 30907934
- PMCID: PMC6563546
- DOI: 10.1001/jamaneurol.2019.0351
Functional Outcome of Intravenous Thrombolysis in Patients With Lacunar Infarcts in the WAKE-UP Trial
Abstract
Importance: The rationale for intravenous thrombolysis in patients with lacunar infarcts is debated, since it is hypothesized that the microvascular occlusion underlying lacunar infarcts might not be susceptible to pharmacological reperfusion treatment.
Objective: To study the efficacy and safety of intravenous thrombolysis among patients with lacunar infarcts.
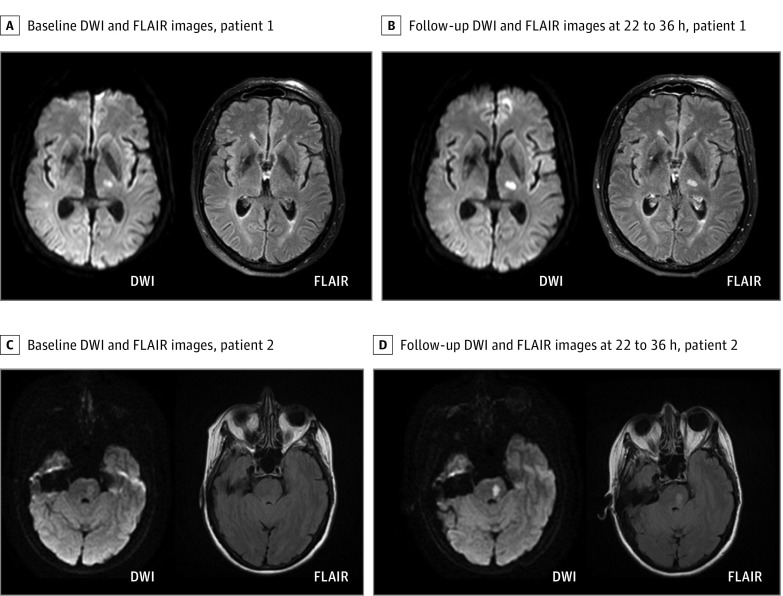
Design, setting, and participants: This exploratory secondary post hoc analysis of the WAKE-UP trial included patients who were screened and enrolled between September 2012 and June 2017 (with final follow-up in September 2017). The WAKE-UP trial was a multicenter, double-blind, placebo-controlled randomized clinical trial to study the efficacy and safety of intravenous thrombolysis with alteplase in patients with an acute stroke of unknown onset time, guided by magnetic resonance imaging. All 503 patients randomized in the WAKE-UP trial were reviewed for lacunar infarcts. Diagnosis of lacunar infarcts was based on magnetic resonance imaging and made by consensus of 2 independent investigators blinded to clinical information.
Main outcomes and measures: The primary efficacy variable was favorable outcome defined by a score of 0 to 1 on the modified Rankin Scale at 90 days after stroke, adjusted for age and severity of symptoms.
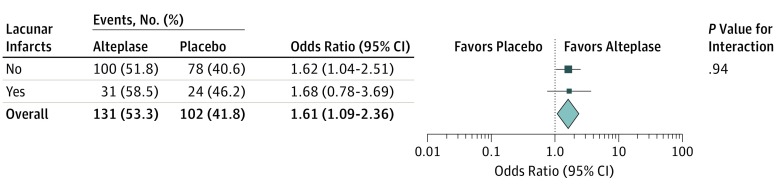
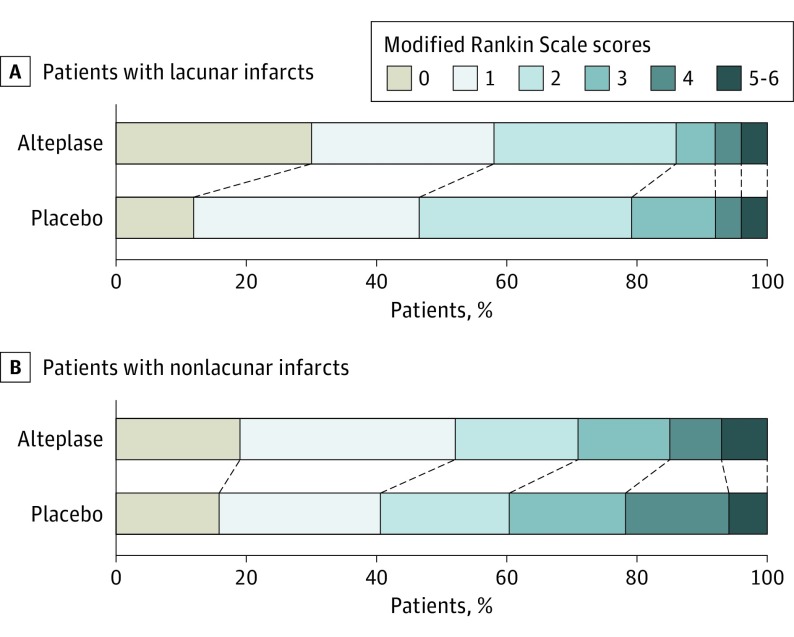
Results: Of the 503 patients randomized in the WAKE-UP trial, 108 patients (including 74 men [68.5%]) had imaging-defined lacunar infarcts, whereas 395 patients (including 251 men [63.5%]) had nonlacunar infarcts. Patients with lacunar infarcts were younger than patients with nonlacunar infarcts (mean age [SD], 63 [12] years vs 66 [12] years; P = .003). Of patients with lacunar infarcts, 55 (50.9%) were assigned to treatment with alteplase and 53 (49.1%) to receive placebo. Treatment with alteplase was associated with higher odds of favorable outcome, with no heterogeneity of treatment outcome between lacunar and nonlacunar stroke subtypes. In patients with lacunar strokes, a favorable outcome was observed in 31 of 53 patients (59%) in the alteplase group compared with 24 of 52 patients (46%) in the placebo group (adjusted odds ratio [aOR], 1.67 [95% CI, 0.77-3.64]). There was 1 death and 1 symptomatic intracranial hemorrhage according to Safe Implementation of Thrombolysis in Stroke-Monitoring Study criteria in the alteplase group, while no death and no symptomatic intracranial hemorrhage occurred in the placebo group. The distribution of the modified Rankin Scale scores 90 days after stroke also showed a nonsignificant shift toward better outcomes in patients with lacunar infarcts treated with alteplase, with an adjusted common odds ratio of 1.94 (95% CI, 0.95-3.93).
Conclusions and relevance: While the WAKE-UP trial was not powered to demonstrate the efficacy of treatment in subgroups of patients, the results indicate that the association of intravenous alteplase with functional outcome does not differ in patients with imaging-defined lacunar infarcts compared with those experiencing other stroke subtypes.
Conflict of interest statement
Figures
Comment in
-
Thrombolysis Works in Lacunar Infarct, Complicating Imaging Selection.JAMA Neurol. 2019 Jun 1;76(6):637-638. doi: 10.1001/jamaneurol.2019.0214. JAMA Neurol. 2019. PMID: 30907930 No abstract available.
References
-
- Sandercock P, Wardlaw JM, Lindley RI, et al. ; IST-3 collaborative group . The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet. 2012;379(9834):2352-2363. doi: 10.1016/S0140-6736(12)60768-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
