

Efficacy and Safety of Intravenous Thrombolysis in Patients with Acute Ischemic Stroke and Pre⁻Existing Disability
- PMID: 30909477
- PMCID: PMC6462959
- DOI: 10.3390/jcm8030400
Efficacy and Safety of Intravenous Thrombolysis in Patients with Acute Ischemic Stroke and Pre⁻Existing Disability
Abstract
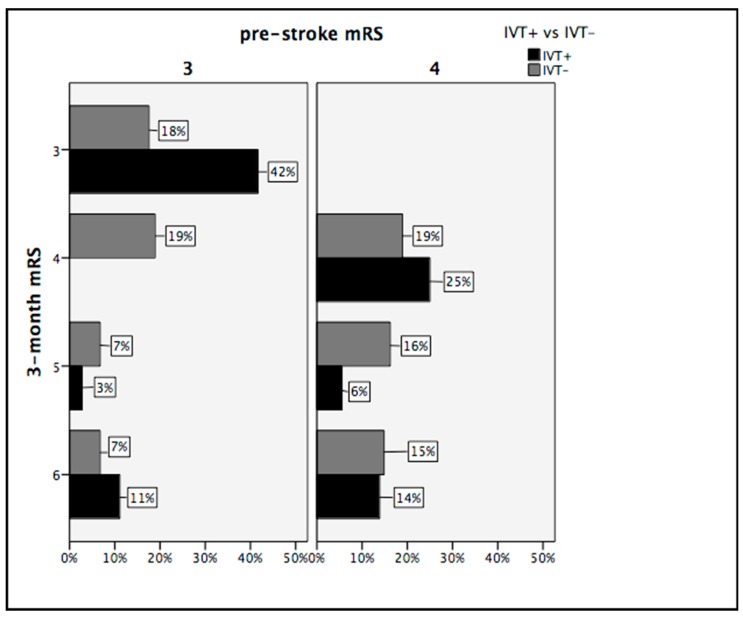
Little is known about intravenous thrombolysis (IVT) in acute ischemic stroke (AIS) patients with pre-existing disability. Disabled patients are often excluded from IVT treatment. Previous studies investigated the role of pre-existing disability on outcomes in AIS patients after IVT. However, no studies have been conducted to date to determine whether IVT may improve clinical outcomes in AIS patients with pre-existing disability. The aim of our study was to evaluate efficacy and safety of IVT in patients with pre-existing moderate and moderately severe disability (pre-stroke modified Rankin Scale score = 3 or 4) affected by AIS. This study was based on a retrospective analysis of a prospectively collected database of consecutive patients admitted to the Udine University Hospital with AIS from January 2015 to May 2018. The efficacy endpoints were the rate of favorable outcome and rate of major neurological improvement. The safety endpoints were the rate of mortality at three months, presence of intracranial hemorrhage (ICH), and presence of symptomatic intracranial hemorrhage (sICH). The study population included 110 AIS patients with pre-existing moderate and moderately severe disability, 36 of which received (IVT+) and 74 did not receive IVT (IVT-). AIS disabled patients treated with IVT had higher rates of favorable outcome (66.7% vs. 36.5%, p = 0.003) and major neurological improvement (39.4% vs. 17.4%, p = 0.01) compared to non-treated ones. Two in three disabled patients returned to their pre-stroke functional status when treated with IVT. Prevalence of three-month mortality, ICH, and sICH did not differ in the two groups. Disabled patients affected by AIS significantly improved after IVT. Moderate and moderately severe disability alone should not be considered, per se, as a contraindication to IVT treatment.
Keywords: acute ischemic stroke; intravenous thrombolysis; modified Rankin Scale; outcomes; pre-existing disability.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- World Health Organization . Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. World Health Organization; Geneva, Switzerland: 2018.
-
- Hay S.I., Abajobir A.A., Abate K.H., Abbafati C., Abbas K.M., Abd-Allah F., Abdulkader R.S., Abdulle A.M., Abebo T.A., Abera S.F., et al. Global, regional, and national disability-adjusted life years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1260–1344. doi: 10.1016/S0140-6736(17)32130-X. - DOI - PMC - PubMed
-
- IST-3 Collaborative Group. Sandercock P., Wardlaw J.M., Lindley R.I., Dennis M., Innes K., Venables G., Czlonkowska A., Kobayashi A., Ricci S., et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the Third International Stroke Trial [IST-3]): A randomised controlled trial. Lancet. 2012;379:2352–2363. doi: 10.1016/S0140-6736(12)60768-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
