

Divergent Six Month Functional Recovery Trajectories and Predictors after Traumatic Brain Injury: Novel Insights from the Citicoline Brain Injury Treatment Trial Study
- PMID: 30909795
- PMCID: PMC6709728
- DOI: 10.1089/neu.2018.6167
Divergent Six Month Functional Recovery Trajectories and Predictors after Traumatic Brain Injury: Novel Insights from the Citicoline Brain Injury Treatment Trial Study
Abstract
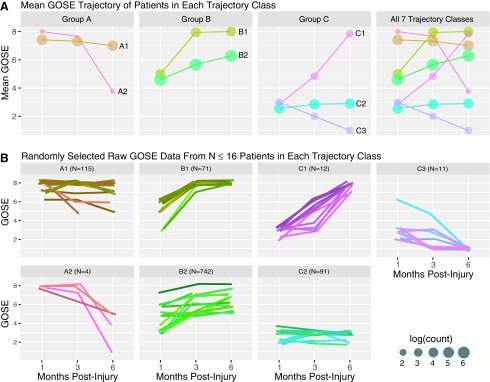
Cross-sectional approaches to outcome assessment may not adequately capture heterogeneity in recovery after traumatic brain injury (TBI). Using latent class mixed models (LCMM), a data-driven analytic that identifies groups of patients with similar trajectories, we identified distinct 6 month functional recovery trajectories in a large cohort (n = 1046) of adults 18-70 years of age with complicated mild to severe TBI who participated in the Citicoline Brain Injury Treatment Trial (COBRIT). We used multinomial logistic fixed effect models and backward elimination, forward selection, and forward stepwise selection with several stopping rules to explore baseline predictors of functional recovery trajectory. Based on statistical and clinical considerations, the seven-class model was deemed superior. Visualization of these seven functional recovery trajectories revealed that each trajectory class started at one of three recovery levels at 1 month, which, for ease of reference we labeled groups A-C: Group A, good recovery (two classes; A1 and A2); Group B, moderate disability (two classes; B1 and B2); and Group C, severe disability (three classes; C1, C2, and C3). By 6 months, these three groups experienced dramatically divergent trajectories. Group A experienced stable good recovery (A1, n = 115) or dramatic decline (A2, n = 4); Group B experienced rapid complete recovery (B1, n = 71) or gradual recovery (B2, n = 742); Group C experienced dramatic rapid recovery (C1, n = 12), no recovery (C2, n = 91), or death (C3, n = 11). Trajectory class membership was not predicted by citicoline treatment (p = 0.57). The models identified demographic, pre-injury, and injury-related predictors of functional recovery trajectory, including: age, race, education, pre-injury employment, pre-injury diabetes, pre-injury psychiatric disorder, site, Glasgow Coma Scale (GCS) score, post-traumatic amnesia, TBI mechanism, major extracranial injury, hemoglobin, and acute computed tomographic (CT) findings. GCS was the most consistently selected predictor across all models. All models also selected at least one demographic or pre-injury medical predictor. LCMM successfully identified dramatically divergent, clinically meaningful 6 month recovery trajectories with utility to inform clinical trial design.
Keywords: TBI; functional outcome; predictors; trajectory.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Finkelstein E., Corso P., and Miller T. (2006). The Incidence and Economic Burden of Inuries in the United States. Oxford University Press: New York
-
- Zafonte R.D., Bagiella E., Ansel B.M., Novack T.A., Friedewald W.T., Hesdorffer D.C., Timmons S.D., Jallo J., Eisenberg H., Hart T., Ricker J.H., Diaz-Arrastia R., Merchant R.E., Temkin N.R., Melton S., and Dikmen S.S. (2012). Effect of citicoline on functional and cognitive status among patients with traumatic brain injury: Citicoline Brain Injury Treatment Trial (COBRIT). JAMA 308, 1993–2000 - PubMed
-
- Wright D.W., Yeatts S.D., Silbergleit R., Palesch Y.Y., Hertzberg V.S., Frankel M., Goldstein F.C., Caveney A.F., Howlett-Smith H., Bengelink E.M., Manley G.T., Merck L.H., Janis L.S., Barsan W.G., and Investigators N. (2014). Very early administration of progesterone for acute traumatic brain injury. N. Engl. J. Med. 371, 2457–2466 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
