

Association of in-hospital resource utilization with post-acute spending in Medicare beneficiaries hospitalized for acute myocardial infarction: a cross-sectional study
- PMID: 30909904
- PMCID: PMC6432744
- DOI: 10.1186/s12913-019-4018-0
Association of in-hospital resource utilization with post-acute spending in Medicare beneficiaries hospitalized for acute myocardial infarction: a cross-sectional study
Abstract
Background: Efforts to decrease hospitalization costs could increase post-acute care costs. This effect could undermine initiatives to reduce overall episode costs and have implications for the design of health care under alternative payment models.
Methods: Among Medicare fee-for-service beneficiaries aged ≥65 years hospitalized with acute myocardial infarction (AMI) between July 2010 and June 2013 in the Premier Healthcare Database, we studied the association of in-hospital and post-acute care resource utilization and outcomes by in-hospital cost tertiles.
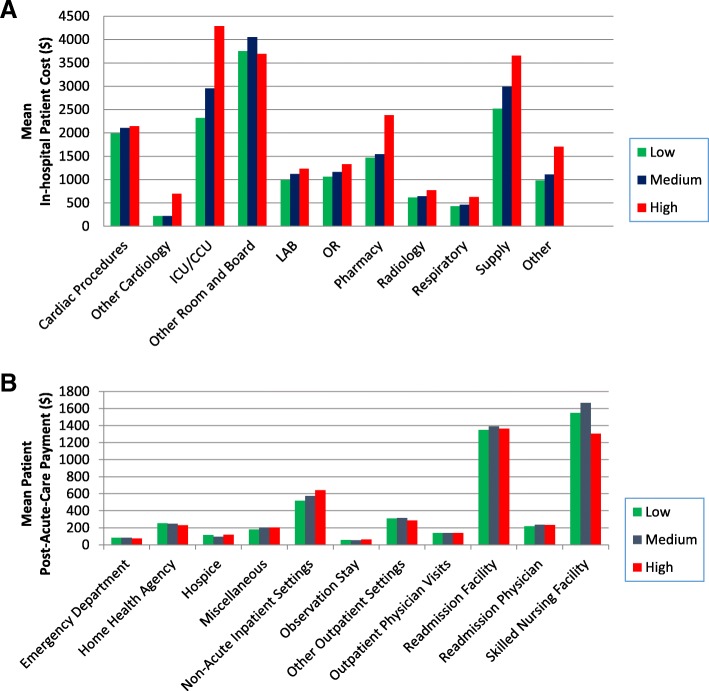
Results: Among patients with AMI at 326 hospitals, the median (range) of each hospital's mean per-patient in-hospital risk-standardized cost (RSC) for the low, medium, and high cost tertiles were $16,257 ($13,097-$17,648), $18,544 ($17,663-$19,875), and $21,831 ($19,923-$31,296), respectively. There was no difference in the median (IQR) of risk-standardized post-acute payments across cost-tertiles: $5014 (4295-6051), $4980 (4349-5931) and $4922 (4056-5457) for the low (n = 90), medium (n = 98), and high (n = 86) in-hospital RSC tertiles (p = 0.21), respectively. In-hospital and 30-day mortality rates did not differ significantly across the in-hospital RSC tertiles; however, 30-day readmission rates were higher at hospitals with higher in-hospital RSCs: median = 17.5, 17.8, and 18.0% at low, medium, and high in-hospital RSC tertiles, respectively (p = 0.005 for test of trend across tertiles).
Conclusions: In our study of patients hospitalized with AMI, greater resource utilization during the hospitalization was not associated with meaningful differences in costs or mortality during the post-acute period. These findings suggest that it may be possible for higher cost hospitals to improve efficiency in care without increasing post-acute care utilization or worsening outcomes.
Keywords: Bundled payments; Costs; Health policy; Medicare; Post-acute.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted under a collaborative contract with Premier, Inc. regarding protection of privacy of hospitals and other providers, which permits the linking of hospital data. For use of Premier data, the Yale University Human Investigation Committee exempted this study protocol as defined by the Office of Human Research Protections because data was de-identified. For CMS data, institutional review board approval, including waiver of the requirement of participant informed consent, was provided by the Yale University Human Investigation Committee.
Consent for publication
Not applicable.
Competing interests
Dr. Krumholz is a recipient of research agreements from Medtronic and Johnson & Johnson (Janssen), through Yale, to develop methods of clinical trial data sharing; was the recipient of a grant from Medtronic and the Food and Drug Administration, through Yale, to develop methods for post-market surveillance of medical devices; received payment from the Arnold & Porter Law Firm for work related to the Sanofi clopidogrel litigation and from the Ben C. Martin Law Firm for work related to the Cook IVC filter litigation; chairs a cardiac scientific advisory board for UnitedHealth; is a participant/participant representative of the IBM Watson Health Life Sciences Board; is a member of the Advisory Boards for Element Science and for Facebook, and the Physician Advisory Board for Aetna; and is the founder of Hugo, a personal health information platform. Drs. Krumholz, Li, Xu, and Desai work under contract to the Centers for Medicare & Medicaid Services to develop and maintain performance measures that are publicly reported. Dr. Lagu has received consulting fees from the Institute for Healthcare Improvement for her input on a project to help health systems achieve disability competence. The other authors do not have disclosures to report.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Association Between 30-Day Episode Payments and Acute Myocardial Infarction Outcomes Among Medicare Beneficiaries.Circ Cardiovasc Qual Outcomes. 2018 Mar;11(3):e004397. doi: 10.1161/CIRCOUTCOMES.117.004397. Circ Cardiovasc Qual Outcomes. 2018. PMID: 29530887 Free PMC article.
-
Association Between Medicare Expenditure Growth and Mortality Rates in Patients With Acute Myocardial Infarction: A Comparison From 1999 Through 2014.JAMA Cardiol. 2018 Feb 1;3(2):114-122. doi: 10.1001/jamacardio.2017.4771. JAMA Cardiol. 2018. PMID: 29261829 Free PMC article.
-
Association Between Medicare Expenditures and Adverse Events for Patients With Acute Myocardial Infarction, Heart Failure, or Pneumonia in the United States.JAMA Netw Open. 2020 Apr 1;3(4):e202142. doi: 10.1001/jamanetworkopen.2020.2142. JAMA Netw Open. 2020. PMID: 32259263 Free PMC article.
-
Association of Medicare Spending With Subspecialty Consultation for Elderly Hospitalized Adults.JAMA Netw Open. 2019 Apr 5;2(4):e191634. doi: 10.1001/jamanetworkopen.2019.1634. JAMA Netw Open. 2019. PMID: 30951157 Free PMC article.
-
Alternative Payment Models and Associations With Stroke Outcomes, Spending, and Service Utilization: A Systematic Review.Stroke. 2022 Jan;53(1):268-278. doi: 10.1161/STROKEAHA.121.033983. Epub 2021 Nov 3. Stroke. 2022. PMID: 34727742
Cited by
-
Association between hospital spending and in-hospital mortality of patients with sepsis based on a Japanese nationwide medical claims database study.Heliyon. 2023 Dec 10;10(1):e23480. doi: 10.1016/j.heliyon.2023.e23480. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38170111 Free PMC article.
-
Examining the Relationship between Cost and Quality of Care in the Neonatal Intensive Care Unit and Beyond.Children (Basel). 2020 Nov 19;7(11):238. doi: 10.3390/children7110238. Children (Basel). 2020. PMID: 33227966 Free PMC article. Review.
References
-
- Tian W. An all-payer view of hospital discharge to postacute care, 2013: statistical brief #205. Healthcare cost and utilization project (HCUP) statistical briefs. Rockville: Agency for Healthcare Research and Quality (US). 2016.; https://www.ncbi.nlm.nih.gov/books/NBK373736/. Accessed 26 Aug 2018.
-
- Interim Report of the Committee on Geographic Variation in Health Care Spending and Promotion of High-Value Health Care: Preliminary committee observations. Washington, DC: The National Academies Press; 2013. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
