

Current epidemiology of cerebrospinal fluid shunt surgery in the UK and Ireland (2004-2013)
- PMID: 30910858
- PMCID: PMC6585267
- DOI: 10.1136/jnnp-2018-319927
Current epidemiology of cerebrospinal fluid shunt surgery in the UK and Ireland (2004-2013)
Abstract
Objectives: To determine current epidemiology and clinical characteristics of cerebrospinal fluid (CSF) shunt surgery, including revisions.
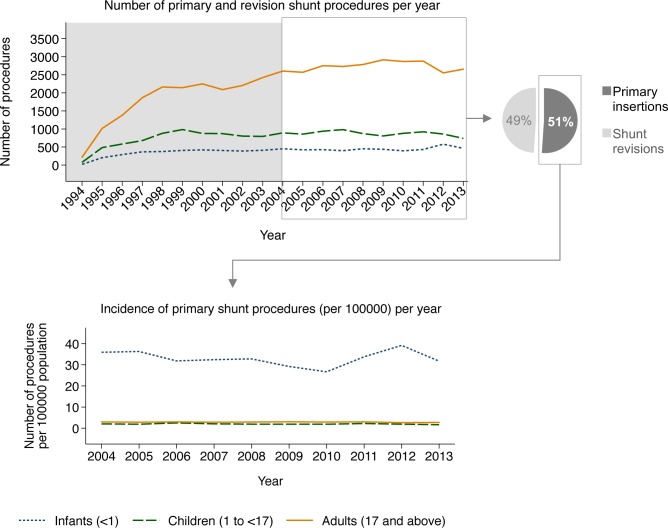
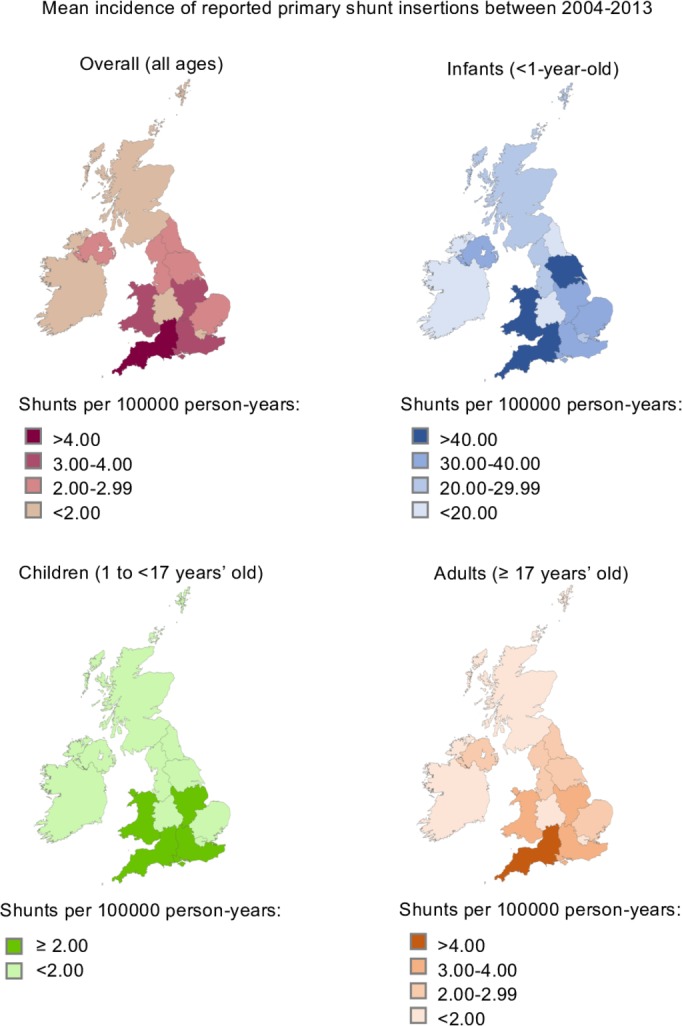
Methods: A retrospective, multicentre, registry-based study was conducted based on 10 years' data from the UK Shunt Registry, including primary and revision shunting procedures reported between 2004 and 2013. Incidence rates of primary shunts, descriptive statistics and shunt revision rates were calculated stratified by age group, geographical region and year of operation.
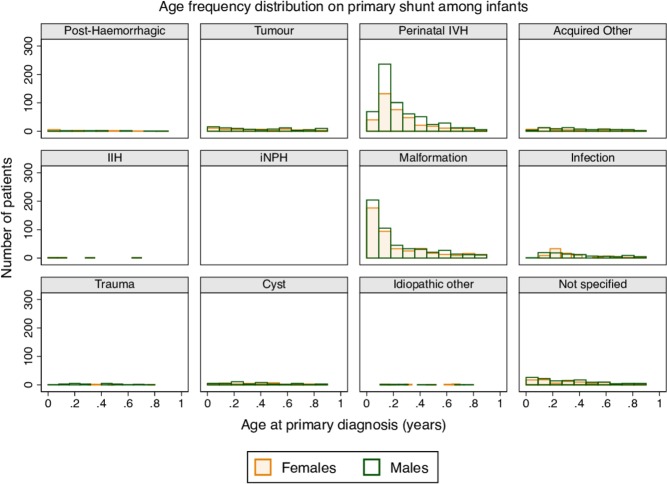
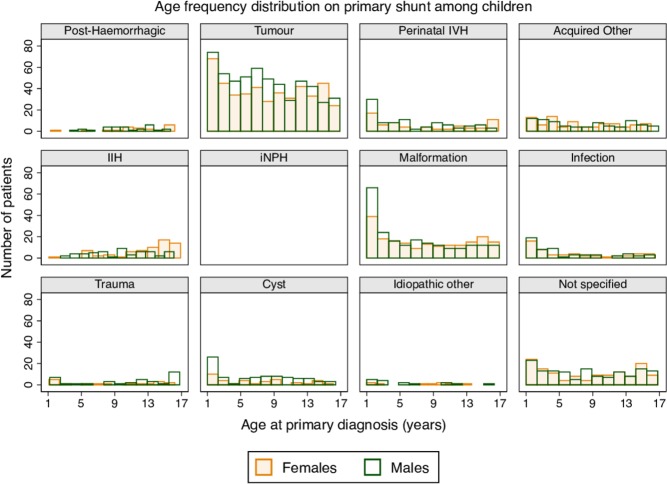
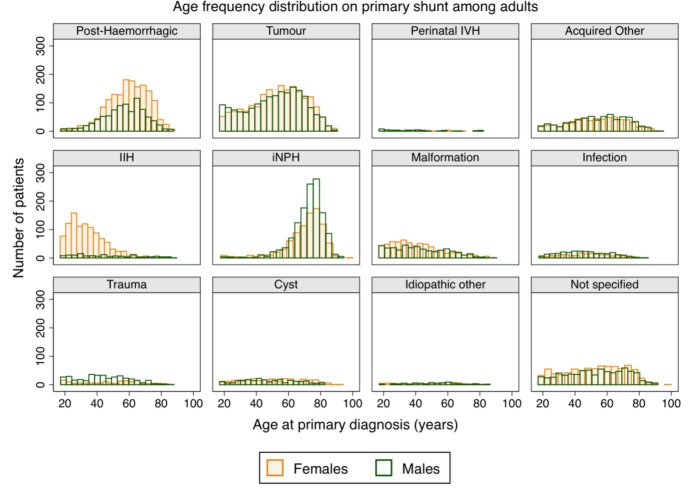
Results: 41 036 procedures in 26 545 patients were submitted during the study period, including 3002 infants, 4389 children and 18 668 adults. Procedures included 20 947 (51.0%) primary shunt insertions in 20 947 patients, and 20 089 (49.0%) revision procedures. Incidence rates of primary shunt insertions for infants, children and adults were 39.5, 2.4 and 3.5 shunts per 100 000 person-years, respectively. These varied by geographical subregion and year of operation. The most common underlying diagnoses were perinatal intraventricular haemorrhage (35.3%) and malformations (33.9%) in infants, tumours (40.5%) and malformations (16.3%) in children, and tumours (24.6%), post-haemorrhagic hydrocephalus (16.2%) and idiopathic normal pressure hydrocephalus (14.2%) in adults. Ninety-day revision rates were 21.9%, 18.6% and 12.8% among infants, children and adults, respectively, while first-year revision rates were 31.0%, 25.2% and 17.4%. The main reasons for revision were underdrainage and infection, but overdrainage and mechanical failure continue to pose problems.
Conclusions: Our report informs patients, carers, clinicians, providers and commissioners of healthcare, researchers and industry of the current epidemiology of shunting for CSF disorders, including the potential risks of complications and frequency of revision.
Keywords: CSF shunting; Epidemiology; Neurosurgery; Registry.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: The UKSR is supported by annual subscription fees from each participating institution. Support for a research fellowship program has been established by industry, who receive data on the performance and usage of their own products to facilitate their post-marketing surveillance. The UK Shunt Registry has complete independence over data collection, analysis and publication. AJJ is supported by an NIHR academic clinical lectureship award. JDP was an NIHR Senior Investigator (2009–2014) and is Honorary Clinical Director of the NIHR Brain Injury Health Technology Co-operative (2012–2017), now MedTech Co-operative (2018–2023). The registry has responsibilities to the Society of British Neurological Surgeons and the Medicines and Healthcare products Regulatory Agency.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources