

Clinical Characteristics and Prognostic Factors of Patients with Intrahepatic Cholangiocarcinoma with Fever: A Propensity Score Matching Analysis
- PMID: 30910867
- PMCID: PMC6656462
- DOI: 10.1634/theoncologist.2018-0268
Clinical Characteristics and Prognostic Factors of Patients with Intrahepatic Cholangiocarcinoma with Fever: A Propensity Score Matching Analysis
Abstract
Background: Patients with intrahepatic cholangiocarcinoma (ICC) rarely present fever as the initial symptom. We aimed to identify clinical characteristics and prognostic factors for these feverish patients.
Subjects, materials, and methods: This study retrospectively reviewed 31 patients with ICC with fever (≥38.0°C) treated at our hospital between January 2002 and December 2014. A propensity score was used to match patients with and without fever at a ratio of 1:2.
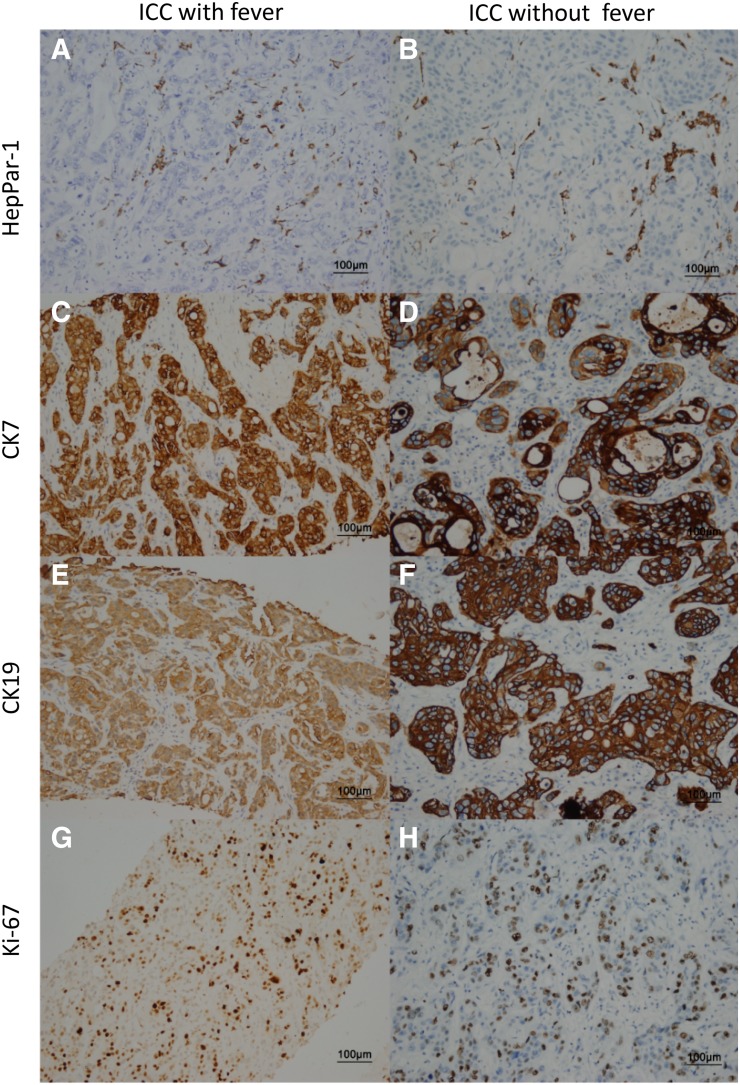
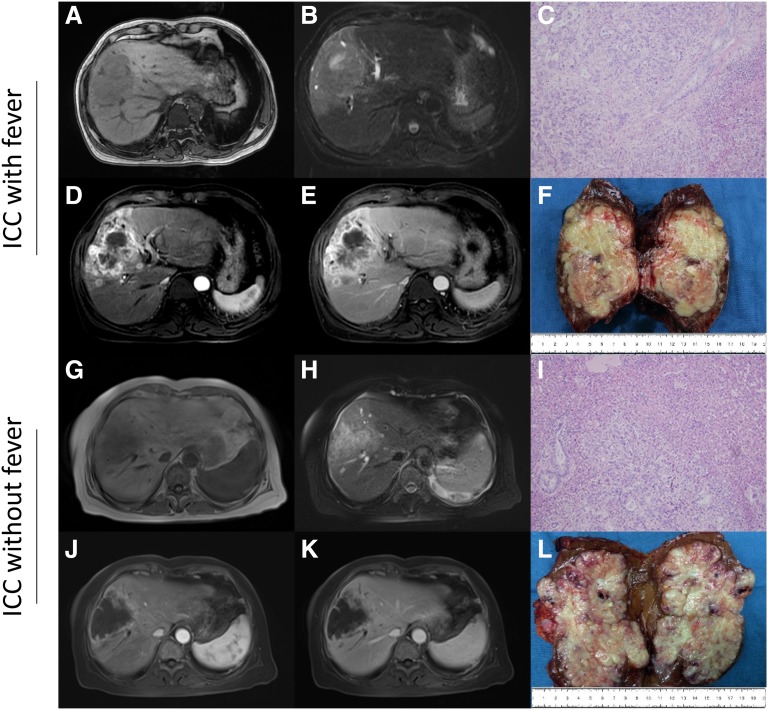
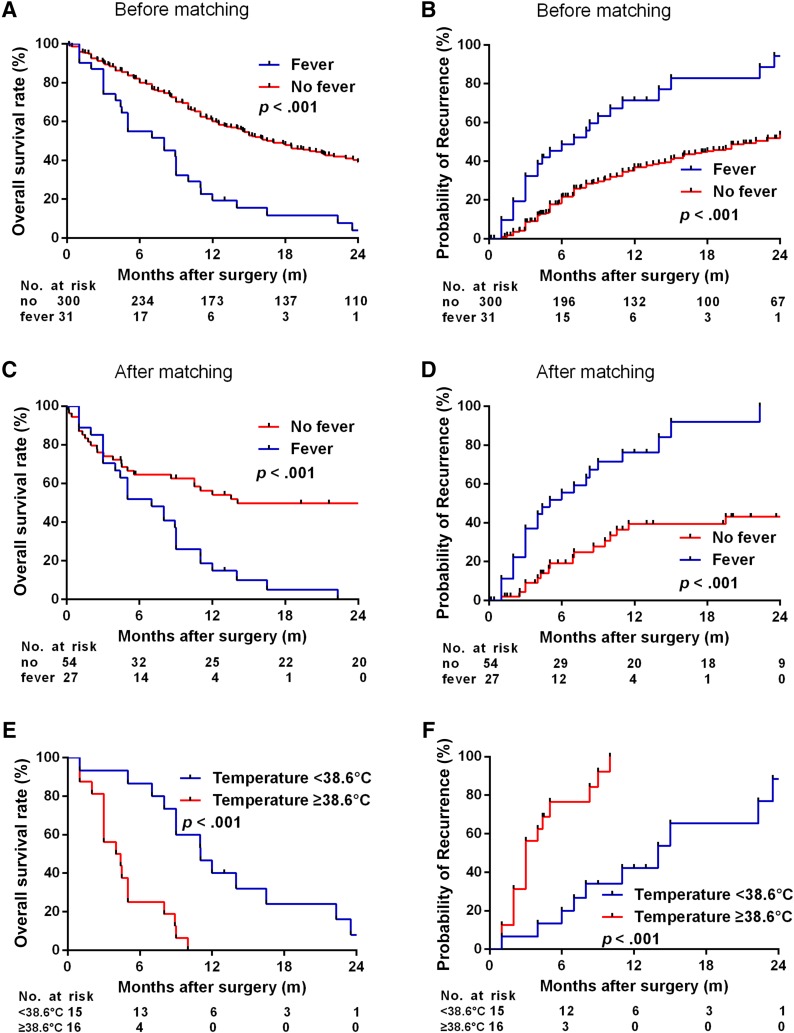
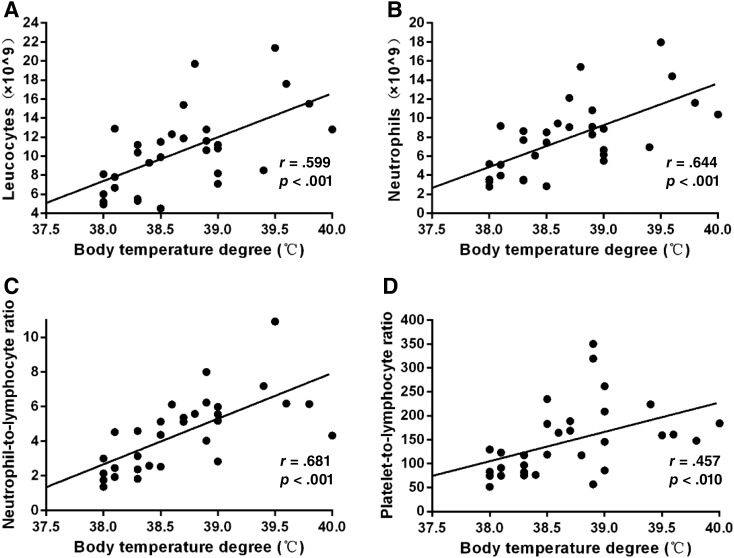
Results: Patients with ICC with fever had higher serum γ-glutamyl transferase and carcinoembryonic antigen levels, larger tumors, poorer tumor differentiation, and worse prognosis (all p < .05) than those without fever. This was supported by propensity score matching (PSM) analysis. Univariate and multivariate analyses indicated that microvascular invasion, hilar lymph node metastasis, and temperature ≥ 38.6°C were related to prognosis. Patients with ICC with fever had higher levels of leucocytes, neutrophils, neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR) in peripheral blood before and after PSM analysis. Body temperature positively correlated with leucocytes (r = 0.599, p < .001), neutrophils (r = 0.644, p < .001), NLR (r = 0.681, p < .001), and PLR (r = 0.457, p = .010).
Conclusion: Patients with ICC with fever ≥38.0°C and ≥38.6°C had poor and extremely poor prognosis, respectively. Radical surgical treatment may improve the prognosis of patients with ICC with fever <38.6°C. However, systemic therapy (e.g., anti-inflammatory and immune therapy) may be preferable to surgery for these patients with fever ≥38.6°C.
Implications for practice: Patients with intrahepatic cholangiocarcinoma (ICC) with fever (≥38.0°C) as the initial symptom are extremely rare. Because their symptoms are similar to those of liver abscess, diagnosis is challenging, and most of these patients are already at an advanced stage at the time of diagnosis. Patients with ICC with fever had different clinical characteristics and worse prognosis than those without fever. The prognosis of those with temperature <38.6°C would be improved by timely surgical intervention. Those with fever ≥38.6°C had an extremely dismal outcome, although they all received radical surgical treatment. New therapeutic strategies are needed to improve survival for patients with ICC with temperature ≥38.6°C.
摘要
背景。肝内胆管癌 (ICC) 患者很少将发热作为首诊症状。我们的目的是确定这些发热患者的临床特征和预后因素。
受试者、材料和方法。本研究回顾性地分析了 2002 年 1 月至 2014 年 12 月期间在我院接受治疗的 31 名伴发热 (≥38.0°C) ICC患者。我们采用倾向评分以 1:2 的比例匹配伴发热与未伴发热的患者。
结果。与未伴发热的ICC患者相比,伴发热ICC患者的血清 γ‐谷氨酰转移酶和癌胚抗原水平较高,肿瘤较大,肿瘤分化较差,预后较差(全部的 p < 0.05)。我们通过倾向评分匹配 (PSM) 分析证实了这一点。单变量和多变量分析表明,微血管浸润、肝门淋巴结转移和体温 ≥38.6°C 与预后有关。伴发热ICC患者在PSM分析之前和之后的白细胞水平、中性粒细胞、中性粒细胞与淋巴细胞的比率 (NLR) 以及外周血中血小板与淋巴细胞的比率 (PLR) 均较高。体温与白细胞(r = 0.599,p < 0.001)、中性粒细胞(r = 0.644,p < 0.001)、NLR(r = 0.681,p < 0.001)以及PLR(r = 0.457,p = 0.010)呈正相关。
结论。体温 ≥38.0°C 和 ≥38.6°C 的伴发热ICC患者的预后效果分别为差和极差。根治性手术治疗可改善体温 <38.6°C 的伴发热ICC患者的预后。但是,对于体温 ≥38.6°C 的伴发热ICC患者,全身治疗(例如抗炎和免疫治疗)可能优于手术治疗。
实践意义:以发热 (≥38.0°C) 为首诊症状的肝内胆管癌(ICC)患者极为少见。由于其症状与肝脓肿相似,给诊断带来了很大的挑战,并且大多数患者在诊断时已处于晚期。伴发热ICC患者的临床特征与未伴发热ICC患者不同,并且预后较差。通过及时的手术干预可以改善体温 <38.6°C 的患者的预后。体温 ≥38.6°C 的发热患者虽然接受了根治性手术治疗,但预后极差。需要新的治疗策略来改善体温 ≥38.6°C 的ICC患者的生存期。
Keywords: Fever; Hepatectomy; Intrahepatic cholangiocarcinoma; Prognosis.
© AlphaMed Press 2019.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Zhang H, Yang T, Wu M et al. Intrahepatic cholangiocarcinoma: Epidemiology, risk factors, diagnosis and surgical management. Cancer Lett 2016;379:198–205. - PubMed
-
- Bridgewater J, Galle PR, Khan SA et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol 2014;60:1268–1289. - PubMed
-
- Esnaola NF, Meyer JE, Karachristos A et al. Evaluation and management of intrahepatic and extrahepatic cholangiocarcinoma. Cancer 2016;122:1349–1369. - PubMed
-
- Li C, Li G, Miao R et al. Primary liver cancer presenting as pyogenic liver abscess: Characteristics, diagnosis, and management. J Surg Oncol 2012;105:687–691. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
