

Pharmacological principles of intraperitoneal and bidirectional chemotherapy
- PMID: 30911633
- PMCID: PMC6405033
- DOI: 10.1515/pp-2017-0010
Pharmacological principles of intraperitoneal and bidirectional chemotherapy
Abstract
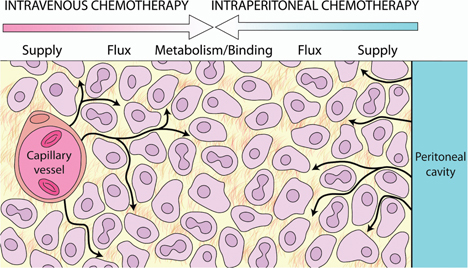
Intraperitoneal chemotherapy is associated with a significant pharmacokinetic and pharmacodynamic benefit and can, alone or in combination with systemic chemotherapy (bidirectional chemotherapy), be used for treating primary and secondary peritoneal surface malignancies. Due to the peritoneal-plasma barrier, high intraperitoneal drug concentration can be achieved by intraperitoneal chemotherapy, whereas systemic concentration remains low. Bidirectional chemotherapy may provide in addition adequate drug concentrations from the side of the subperitoneal space to the peritoneal tumour nodules. Major pharmacological problems of intraperitoneal chemotherapy are limited tissue penetration and poor homogeneity of drug distribution to the entire seroperitoneal surface. Significant pharmacological determinants of intraperitoneal chemotherapy are choice of drug, drug dosage, solution volume, carrier solution, intra-abdominal pressure, temperature, duration, mode of administration, extent of peritonectomy and interindividual variability. Drugs most commonly applied for intraperitoneal chemotherapy include mitomycin C, cisplatin, carboplatin, oxaliplatin, irinotecan, 5-fluoruracil, gemcitabine, paclitaxel, docetaxel, doxorubicin, premetrexed and melphalan. The drugs and their doses that are used vary widely among centres. While the adequate drug choice for intraperitoneal and bidirectional chemotherapy is essential, randomized clinical trials to determine the most optimal drug or drug combination are lacking, and only eight retrospective comparative clinical studies are available. Further clinical pharmacological studies are required to determine the most effective drug regimen for intraperitoneal and bidirectional chemotherapy in various indications. In the future, reliable drug sensitivity testing and genetic profiling of peritoneal metastases will be needed for enabling patient-specific therapy.
Keywords: intraperitoneal chemotherapy; peritoneal metastases; peritoneal surface malignancy; pharmacodynamics; pharmacokinetics; pharmacology.
Conflict of interest statement
Competing interests: The funding organization(s) played no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the report for publication.
Figures
References
-
- Sugarbaker PH, Stuart OA, Vidal-Jove J, Pessagno AM, DeBruijn EA. Pharmacokinetics of the peritoneal–plasma barrier after systemic mitomycin C administration. Cancer Treat Res 1996;82:41–52. - PubMed
-
- Weisberger AS, Levine B, Storaasli JP. Use of nitrogen mustard in treatment of serous effusions of neoplastic origin. J Am Med Assoc 1955;159:1704–7. - PubMed
-
- De Bree E, Tsiftsis DD. Principles of perioperative intraperitoneal chemotherapy for peritoneal carcinomatosis. Recent Results Cancer Res 2007;169:39–51. - PubMed
-
- De Bree E, Tsiftsis DD. Experimental and pharmacokinetic studies in intraperitoneal chemotherapy: From laboratory bench to bedside. Recent Results Cancer Res 2007;169:53–73. - PubMed
-
- Flessner MF. The transport barrier in intraperitoneal therapy. Am J Physiol Renal Physiol 2005;288:F433–42. - PubMed
Publication types
LinkOut - more resources
Full Text Sources