

Effect of Sustained Inflations vs Intermittent Positive Pressure Ventilation on Bronchopulmonary Dysplasia or Death Among Extremely Preterm Infants: The SAIL Randomized Clinical Trial
- PMID: 30912836
- PMCID: PMC6439695
- DOI: 10.1001/jama.2019.1660
Effect of Sustained Inflations vs Intermittent Positive Pressure Ventilation on Bronchopulmonary Dysplasia or Death Among Extremely Preterm Infants: The SAIL Randomized Clinical Trial
Abstract
Importance: Preterm infants must establish regular respirations at delivery. Sustained inflations may establish lung volume faster than short inflations.
Objective: To determine whether a ventilation strategy including sustained inflations, compared with standard intermittent positive pressure ventilation, reduces bronchopulmonary dysplasia (BPD) or death at 36 weeks' postmenstrual age without harm in extremely preterm infants.
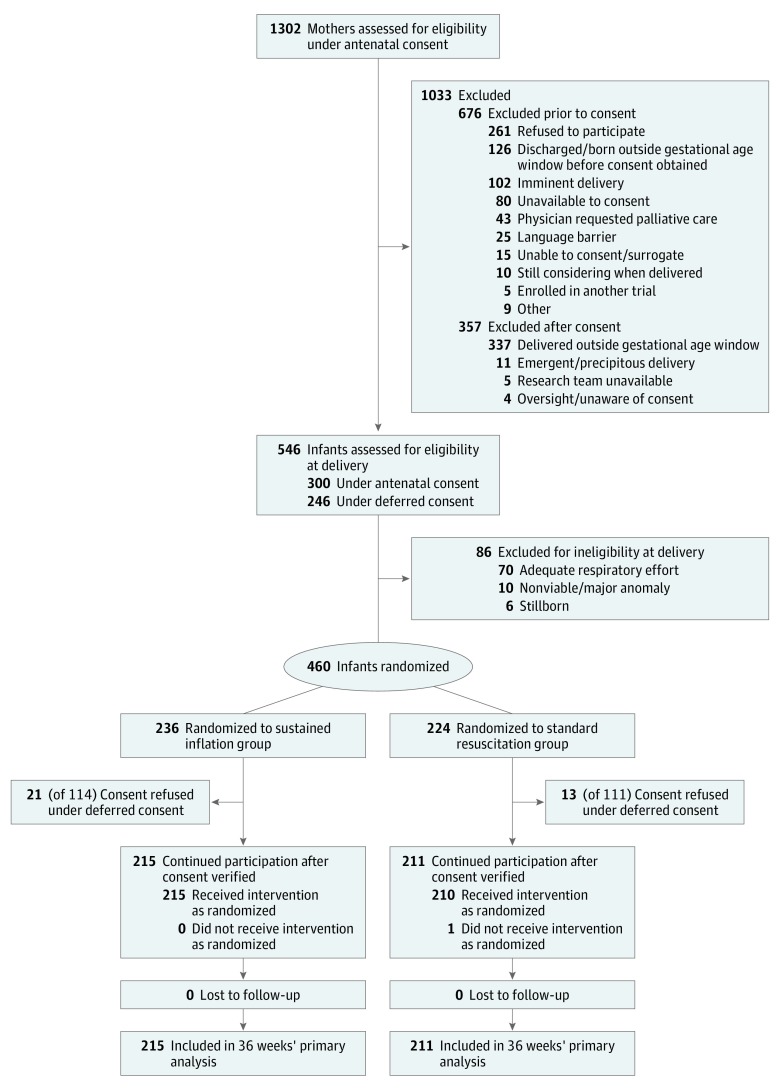
Design, setting, and participants: Unmasked, randomized clinical trial (August 2014 to September 2017, with follow-up to February 15, 2018) conducted in 18 neonatal intensive care units in 9 countries. Preterm infants 23 to 26 weeks' gestational age requiring resuscitation with inadequate respiratory effort or bradycardia were enrolled. Planned enrollment was 600 infants. The trial was stopped after enrolling 426 infants, following a prespecified review of adverse outcomes.
Interventions: The experimental intervention was up to 2 sustained inflations at maximal peak pressure of 25 cm H2O for 15 seconds using a T-piece and mask (n = 215); standard resuscitation was intermittent positive pressure ventilation (n = 211).
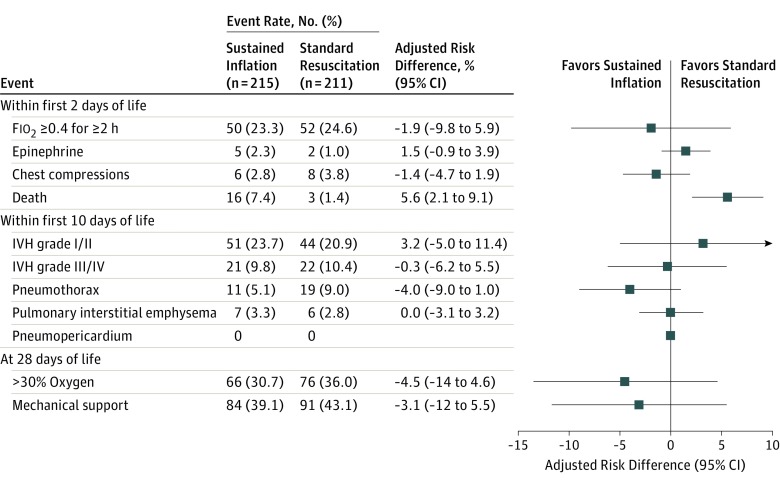
Main outcome and measures: The primary outcome was the rate of BPD or death at 36 weeks' postmenstrual age. There were 27 prespecified secondary efficacy outcomes and 7 safety outcomes, including death at less than 48 hours.
Results: Among 460 infants randomized (mean [SD] gestational age, 25.30 [0.97] weeks; 50.2% female), 426 infants (92.6%) completed the trial. In the sustained inflation group, 137 infants (63.7%) died or survived with BPD vs 125 infants (59.2%) in the standard resuscitation group (adjusted risk difference [aRD], 4.7% [95% CI, -3.8% to 13.1%]; P = .29). Death at less than 48 hours of age occurred in 16 infants (7.4%) in the sustained inflation group vs 3 infants (1.4%) in the standard resuscitation group (aRD, 5.6% [95% CI, 2.1% to 9.1%]; P = .002). Blinded adjudication detected an imbalance of rates of early death possibly attributable to resuscitation (sustained inflation: 11/16; standard resuscitation: 1/3). Of 27 secondary efficacy outcomes assessed by 36 weeks' postmenstrual age, 26 showed no significant difference between groups.
Conclusions and relevance: Among extremely preterm infants requiring resuscitation at birth, a ventilation strategy involving 2 sustained inflations, compared with standard intermittent positive pressure ventilation, did not reduce the risk of BPD or death at 36 weeks' postmenstrual age. These findings do not support the use of ventilation with sustained inflations among extremely preterm infants, although early termination of the trial limits definitive conclusions.
Trial registration: clinicaltrials.gov Identifier: NCT02139800.
Conflict of interest statement
Figures
Comment in
-
Delivery Room Resuscitation of Extremely Preterm Infants.JAMA. 2019 Mar 26;321(12):1161-1162. doi: 10.1001/jama.2019.2010. JAMA. 2019. PMID: 30912816 No abstract available.
-
Sustained lung inflation does not decrease bronchopulmonary dysplasia or death among extremely preterm infants: A Commentary on The SAIL randomised clinical trial.Acta Paediatr. 2019 Nov;108(11):2113-2114. doi: 10.1111/apa.14949. Epub 2019 Aug 23. Acta Paediatr. 2019. PMID: 31442317 No abstract available.
References
-
- Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for preventing morbidity and mortality in very preterm infants. Cochrane Database Syst Rev. 2016;(6):CD001243. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
