

SMARThealth India: A stepped-wedge, cluster randomised controlled trial of a community health worker managed mobile health intervention for people assessed at high cardiovascular disease risk in rural India
- PMID: 30913216
- PMCID: PMC6435227
- DOI: 10.1371/journal.pone.0213708
SMARThealth India: A stepped-wedge, cluster randomised controlled trial of a community health worker managed mobile health intervention for people assessed at high cardiovascular disease risk in rural India
Abstract
Background: Cardiovascular diseases (CVD) are rising in India resulting in major health system challenges.
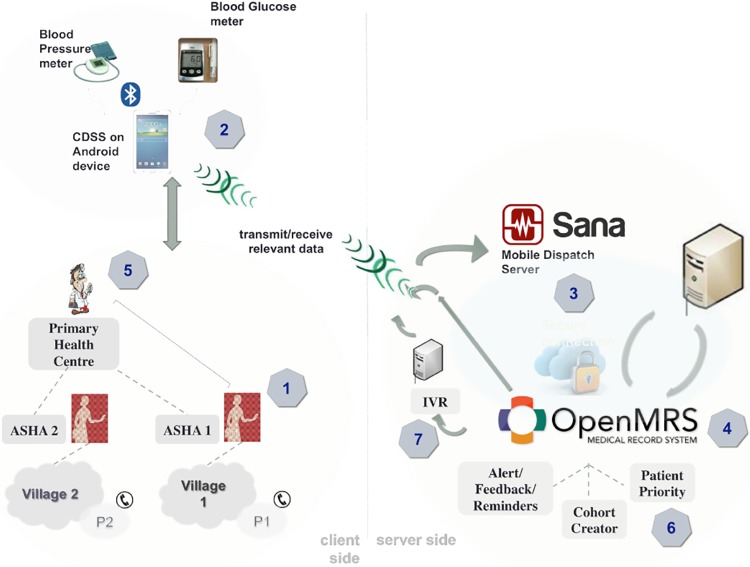
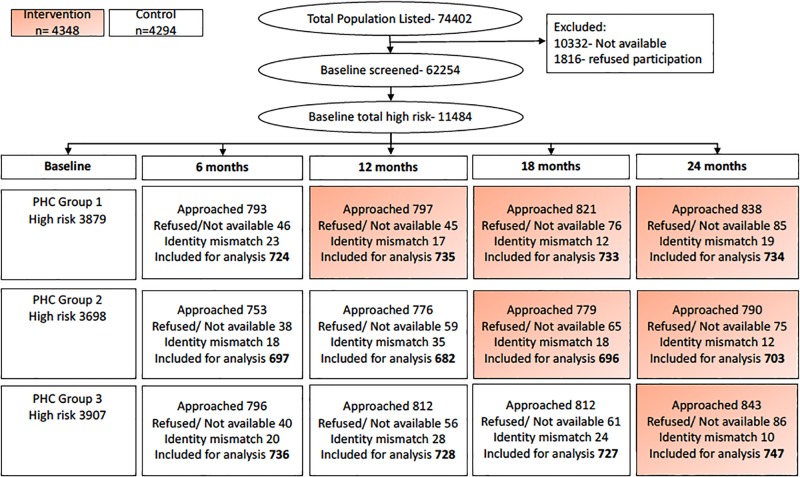
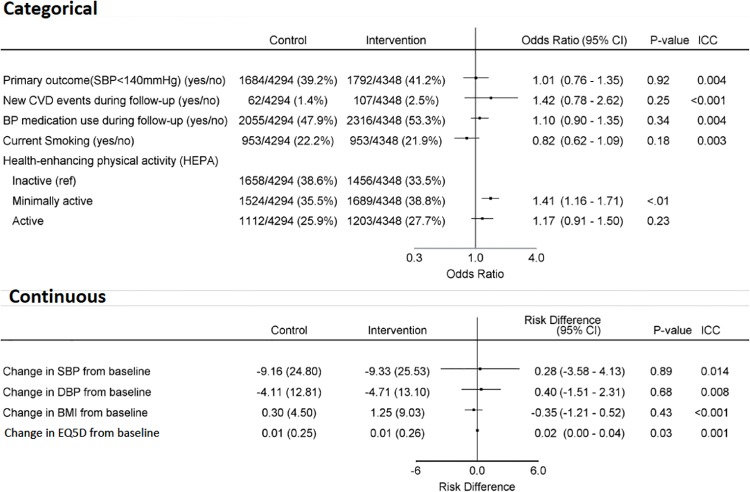
Methods: Eighteen primary health centre (PHC) clusters in rural Andhra Pradesh were randomised over three, 6-month steps to an intervention comprising: (1) household CVD risk assessments by village-based community health workers (CHWs) using a mobile tablet device; (2) electronic referral and clinical decision support for PHC doctors; and (3) a tracking system for follow-up care. Independent data collectors screened people aged ≥ 40 years in 54 villages serviced by the PHCs to create a high CVD risk cohort (based on WHO risk charts and blood pressure thresholds). Randomly selected, independent samples, comprising 15% of this cohort, were reviewed at each 6-month step. The primary outcome was the proportion meeting systolic blood pressure (SBP) targets (<140mmHg).
Findings: Eight-four percent of the eligible population (n = 62,254) were assessed at baseline (18.4% at high CVD risk). Of those at high risk, 75.3% were followed up over two years. CHWs screened 85.9% of the baseline cohort and doctors followed up 70.0% of all high risk referrals. There was no difference in the proportion of people achieving SBP targets (41.2% vs 39.2%; adjusted odds ratio (OR) 1.01 95% CI 0.76-1.35) or receiving BP-lowering medications in the intervention vs control periods respectively. There was a high discordance in risk scores generated by independent data collectors and CHWs, resulting in only 37.2% of the evaluation cohort exposed to the intervention. This discordance was mainly driven by fluctuating BP values (both normal variability and marked seasonal variations). In the pre-specified high risk concordant subgroup, there was greater use of BP-lowering medications in the intervention period (54.3% vs 47.9%, OR 1.22, 95% CI 1.03-1.44) but no impact on BP control.
Conclusions: The strategy was well implemented with increased treatment rates among high risk individuals assessed by CHWs, however effects on BP were not demonstrated. Use of guideline-recommended BP thresholds for identifying high risk individuals substantially affected the reproducibility of risk assessment, and thus the ability to reliably evaluate the effectiveness of the intervention. In addition, unanticipated seasonal variation in BP in the context of a stepped-wedge trial highlights the inherent risks of this study design.
Trial registration: Clinical Trials Registry of India CTRI/2013/06/ 003753.
Conflict of interest statement
The authors have declared that no competing interests exist. The George Institute for Global Health has a wholly owned social enterprise that is conducting commercial projects that include aspects of the intervention tested in this study.
Figures
References
-
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet. 2015;385(9963):117–71. 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
-
- Patel V, Chatterji S, Chisholm D, Ebrahim S, Gopalakrishna G, Mathers C, et al. Chronic diseases and injuries in India. The Lancet. 2011;377(9763):413–28. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
