

Structural weakening of the colonic mucus barrier is an early event in ulcerative colitis pathogenesis
- PMID: 30914450
- PMCID: PMC6872445
- DOI: 10.1136/gutjnl-2018-317571
Structural weakening of the colonic mucus barrier is an early event in ulcerative colitis pathogenesis
Abstract
Objective: The colonic inner mucus layer protects us from pathogens and commensal-induced inflammation, and has been shown to be defective in active UC. The aim of this study was to determine the underlying compositional alterations, their molecular background and potential contribution to UC pathogenesis.
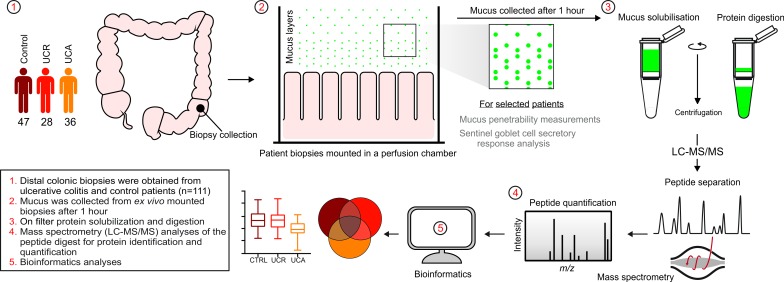
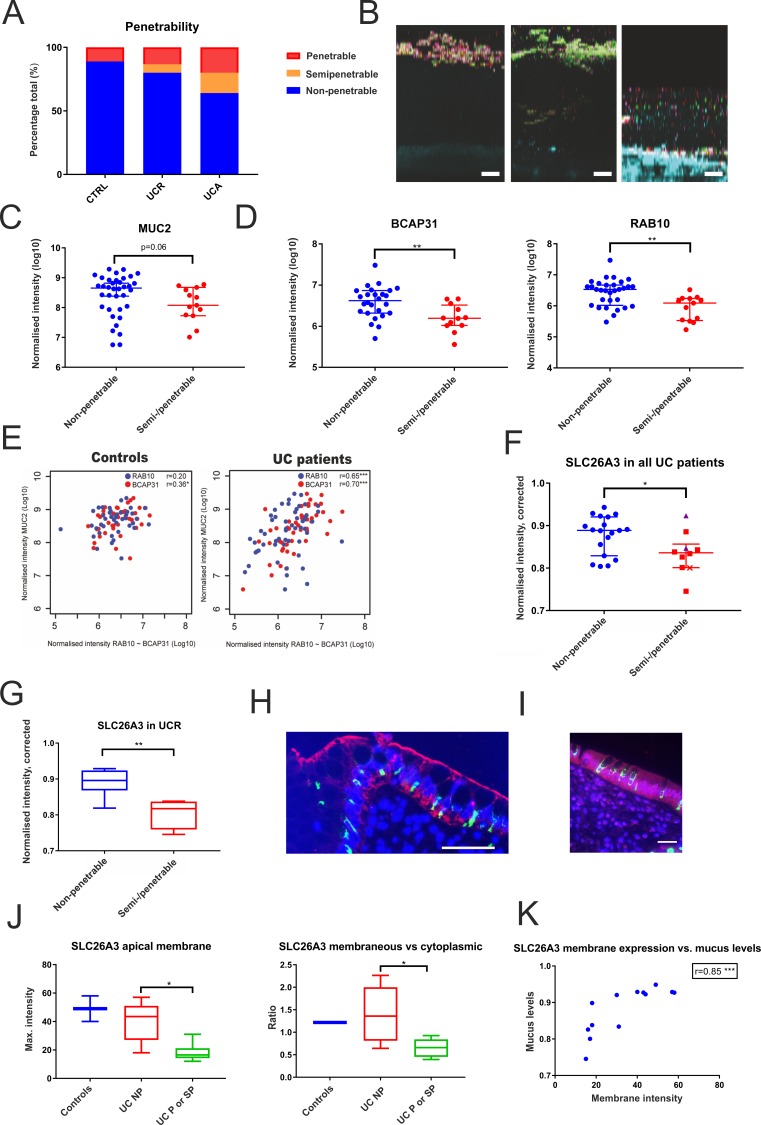
Design: In this single-centre case-control study, sigmoid colon biopsies were obtained from patients with UC with ongoing inflammation (n=36) or in remission (n=28), and from 47 patients without colonic disease. Mucus samples were collected from biopsies ex vivo, and their protein composition analysed by nanoliquid chromatography-tandem mass spectrometry. Mucus penetrability and goblet cell responses to microbial stimulus were assessed in a subset of patients.
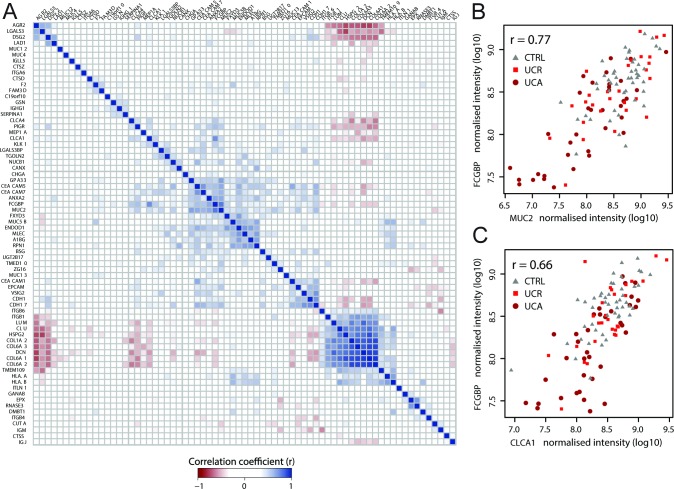
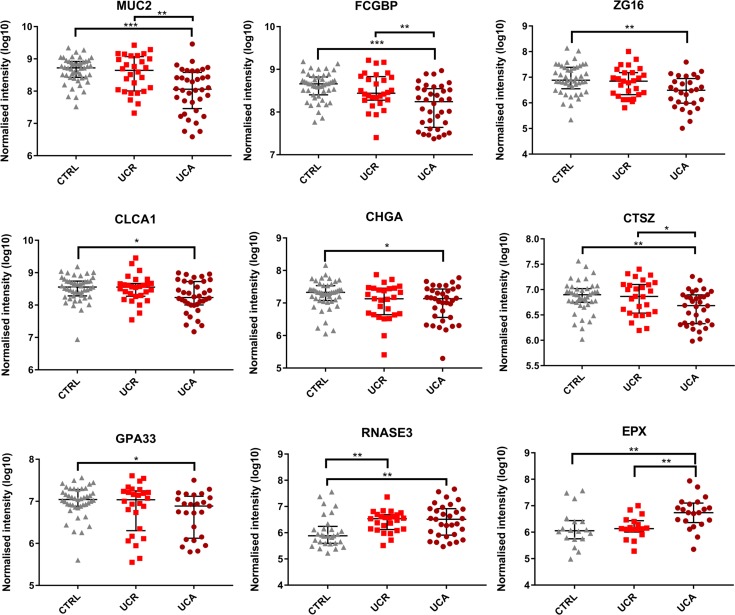
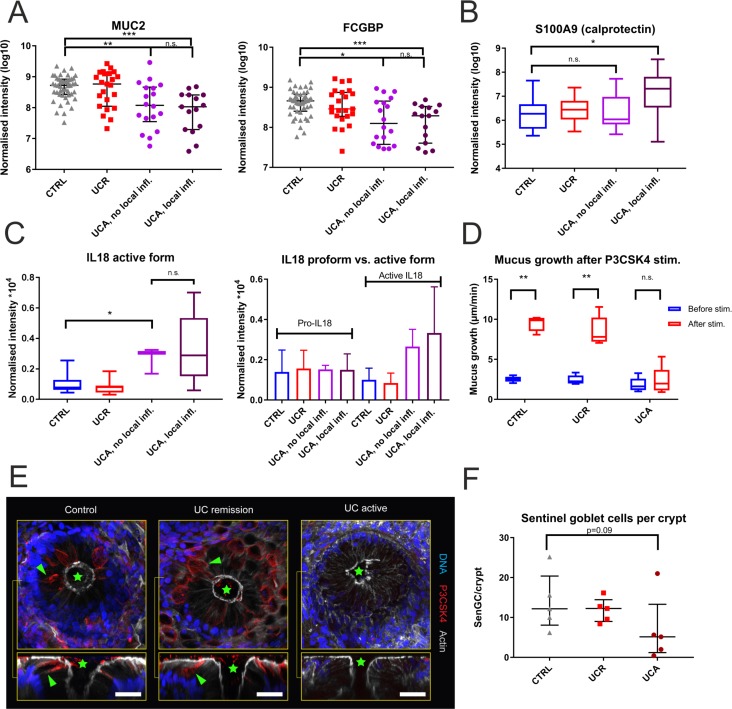
Results: The core mucus proteome was found to consist of a small set of 29 secreted/transmembrane proteins. In active UC, major structural mucus components including the mucin MUC2 (p<0.0001) were reduced, also in non-inflamed segments. Active UC was associated with decreased numbers of sentinel goblet cells and attenuation of the goblet cell secretory response to microbial challenge. Abnormal penetrability of the inner mucus layer was observed in a subset of patients with UC (12/40; 30%). Proteomic alterations in penetrable mucus samples included a reduction of the SLC26A3 apical membrane anion exchanger, which supplies bicarbonate required for colonic mucin barrier formation.
Conclusion: Core mucus structural components were reduced in active UC. These alterations were associated with attenuation of the goblet cell secretory response to microbial challenge, but occurred independent of local inflammation. Thus, mucus abnormalities are likely to contribute to UC pathogenesis.
Keywords: mucins; mucosal barrier; mucosal protection; mucus; ulcerative colitis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous