

The unexplained success of stentplasty vasospasm treatment : Insights using Mechanistic Mathematical Modeling
- PMID: 30915482
- PMCID: PMC7158575
- DOI: 10.1007/s00062-019-00776-2
The unexplained success of stentplasty vasospasm treatment : Insights using Mechanistic Mathematical Modeling
Erratum in
-
Correction to: The unexplained success of stentplasty vasospasm treatment : Insights using Mechanistic Mathematical Modeling.Clin Neuroradiol. 2019 Dec;29(4):775. doi: 10.1007/s00062-019-00782-4. Clin Neuroradiol. 2019. PMID: 31020336 Free PMC article.
Abstract
Background: Cerebral vasospasm (CVS) following subarachnoid hemorrhage occurs in up to 70% of patients. Recently, stents have been used to successfully treat CVS. This implies that the force required to expand spastic vessels and resolve vasospasm is lower than previously thought.
Objective: We develop a mechanistic model of the spastic arterial wall to provide insight into CVS and predict the forces required to treat it.
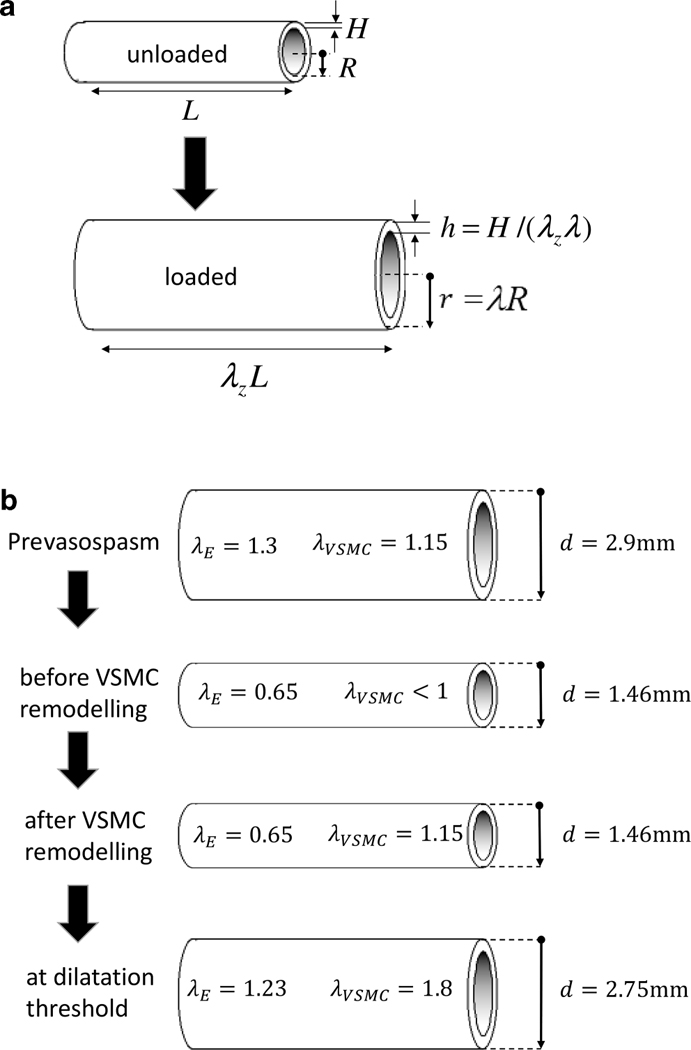
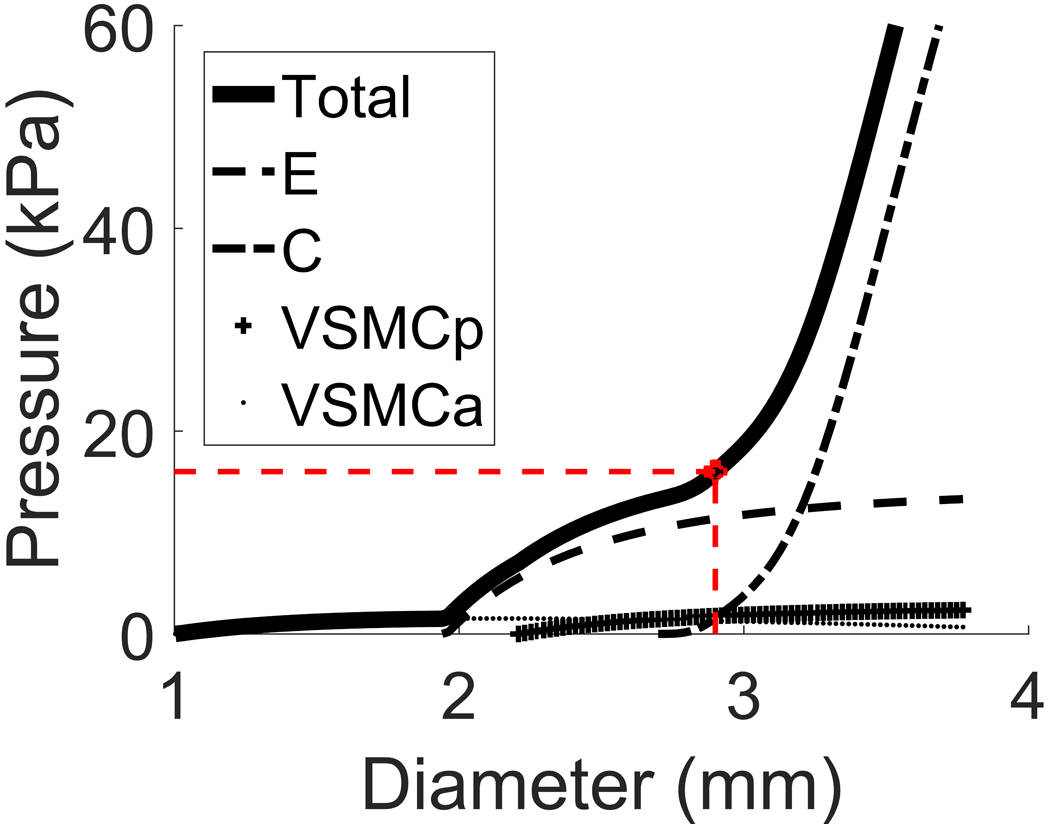
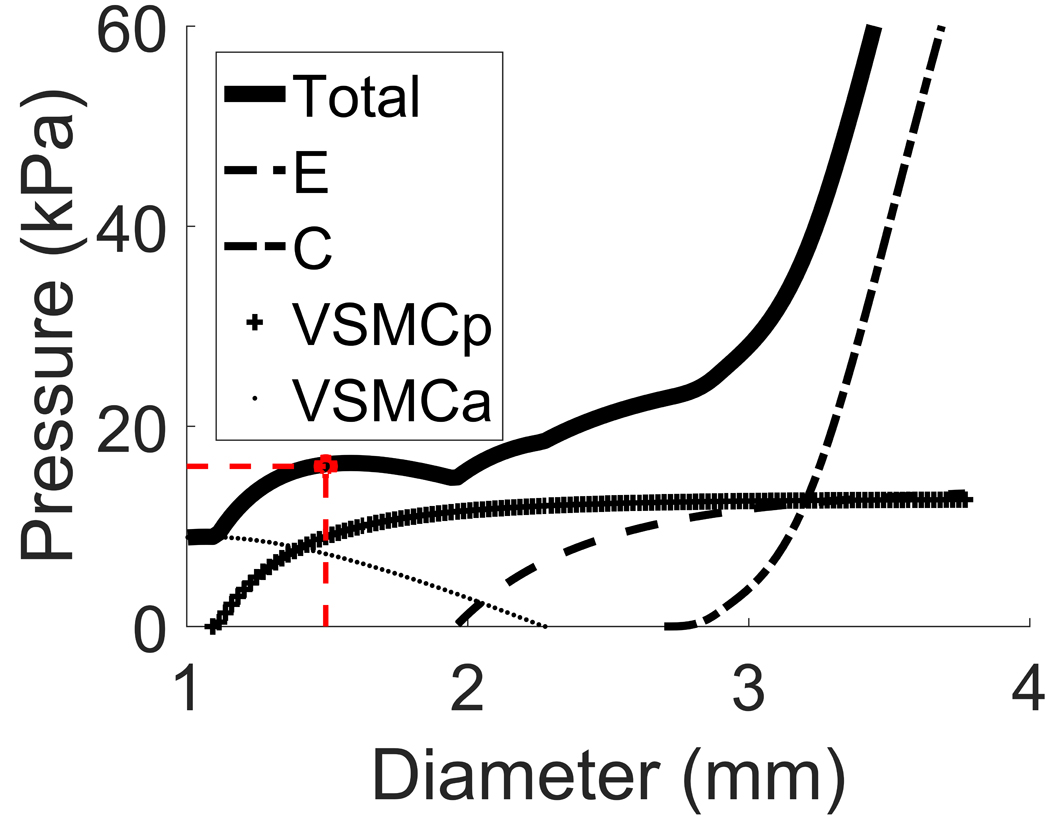
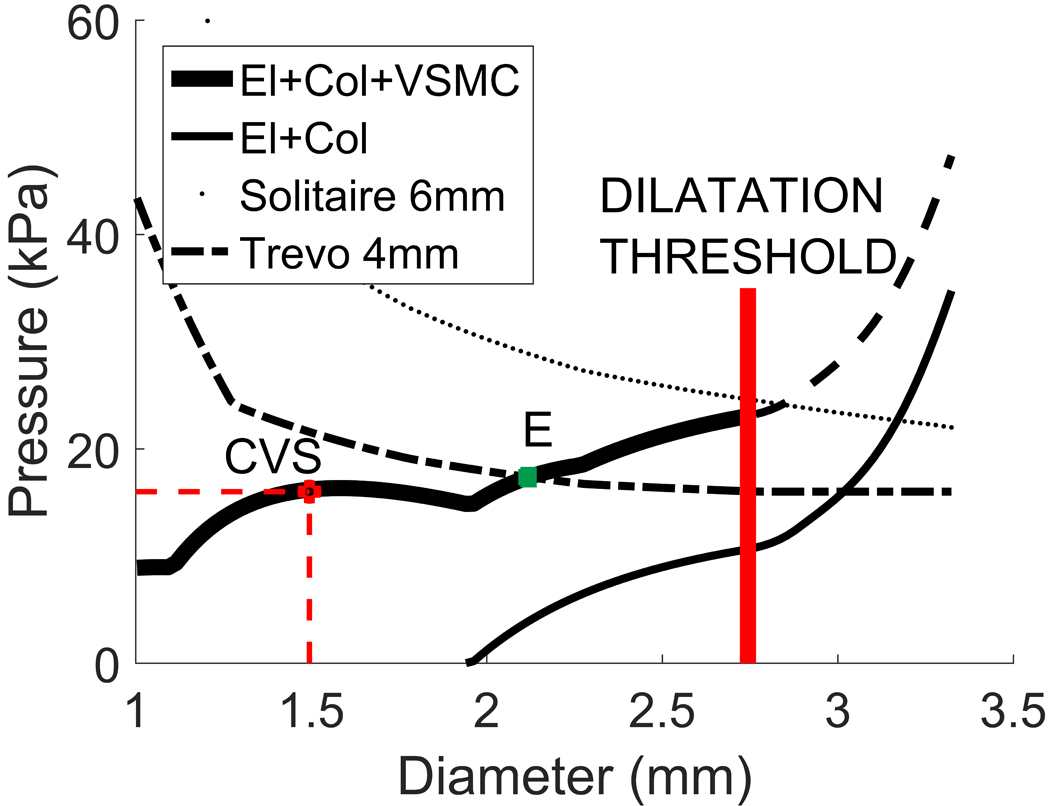
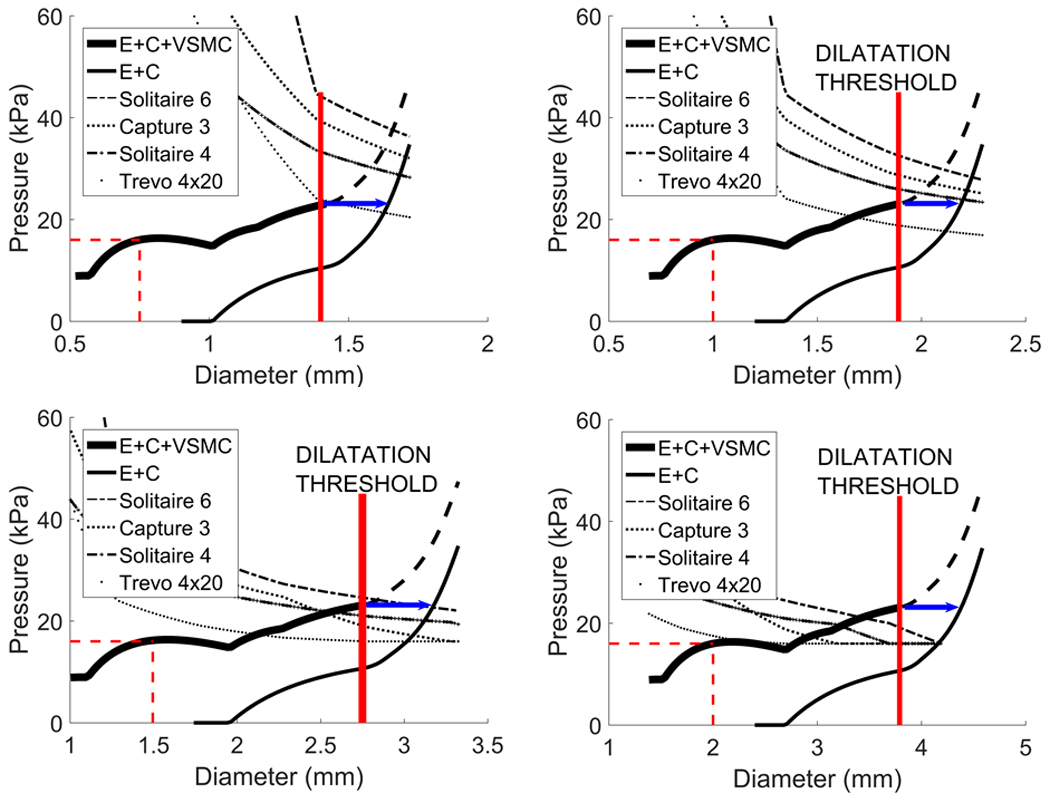
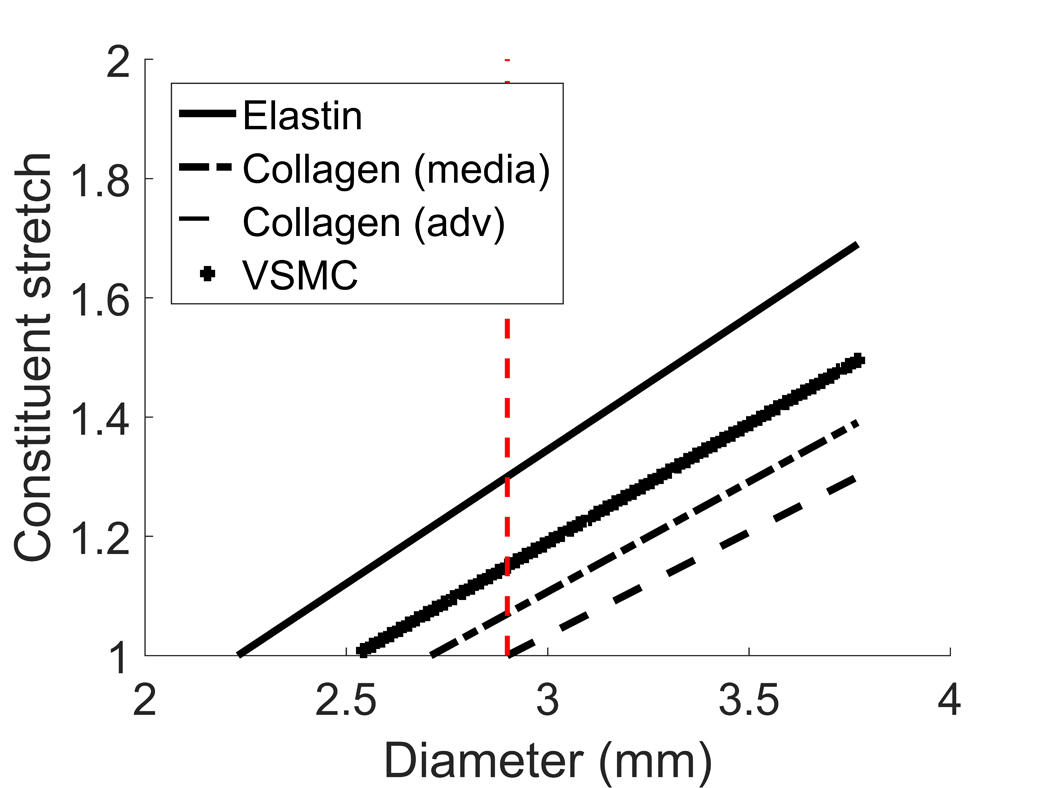
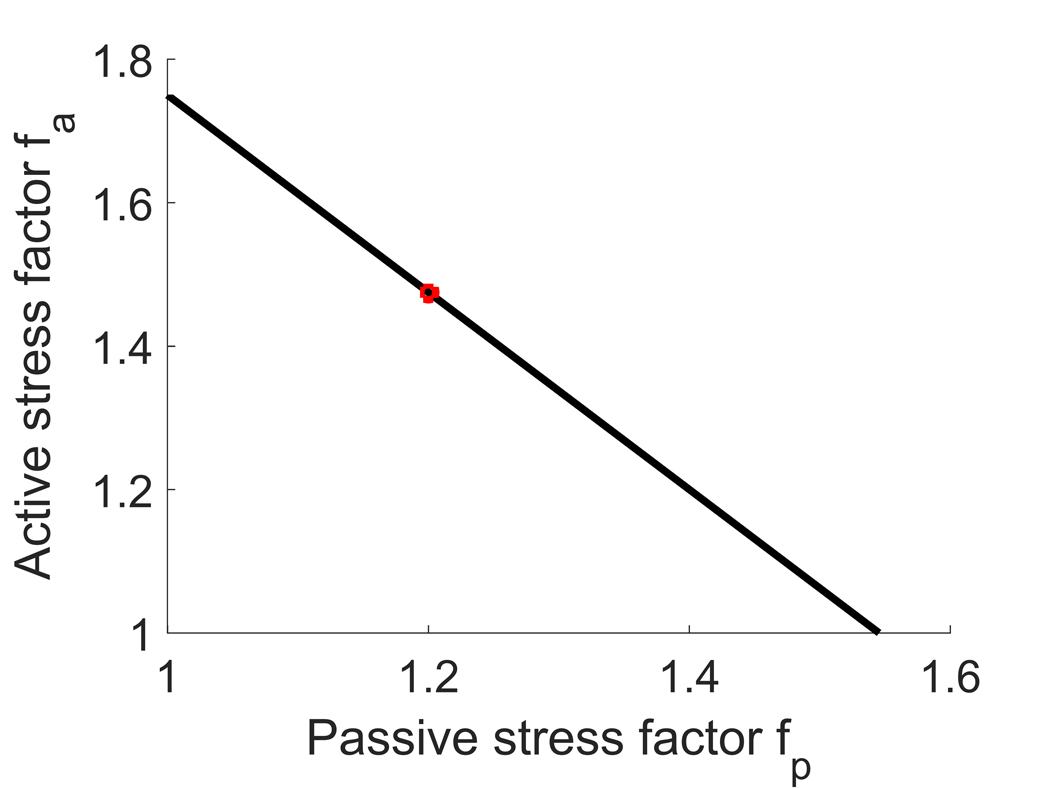
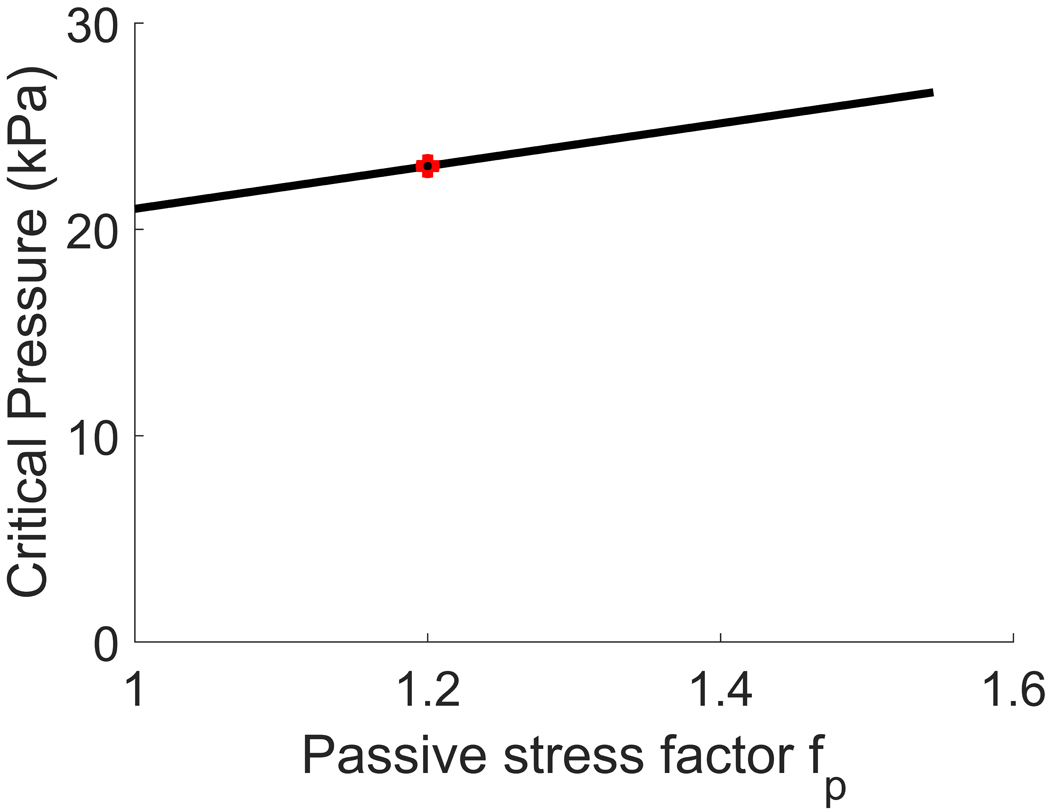
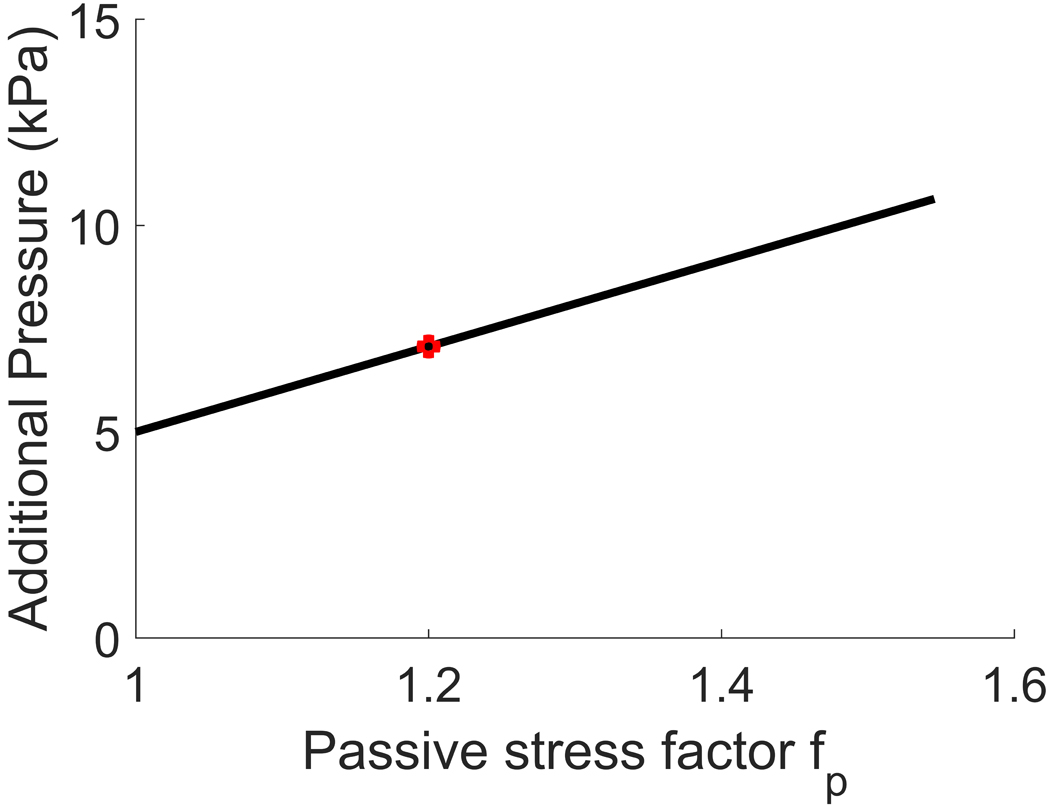
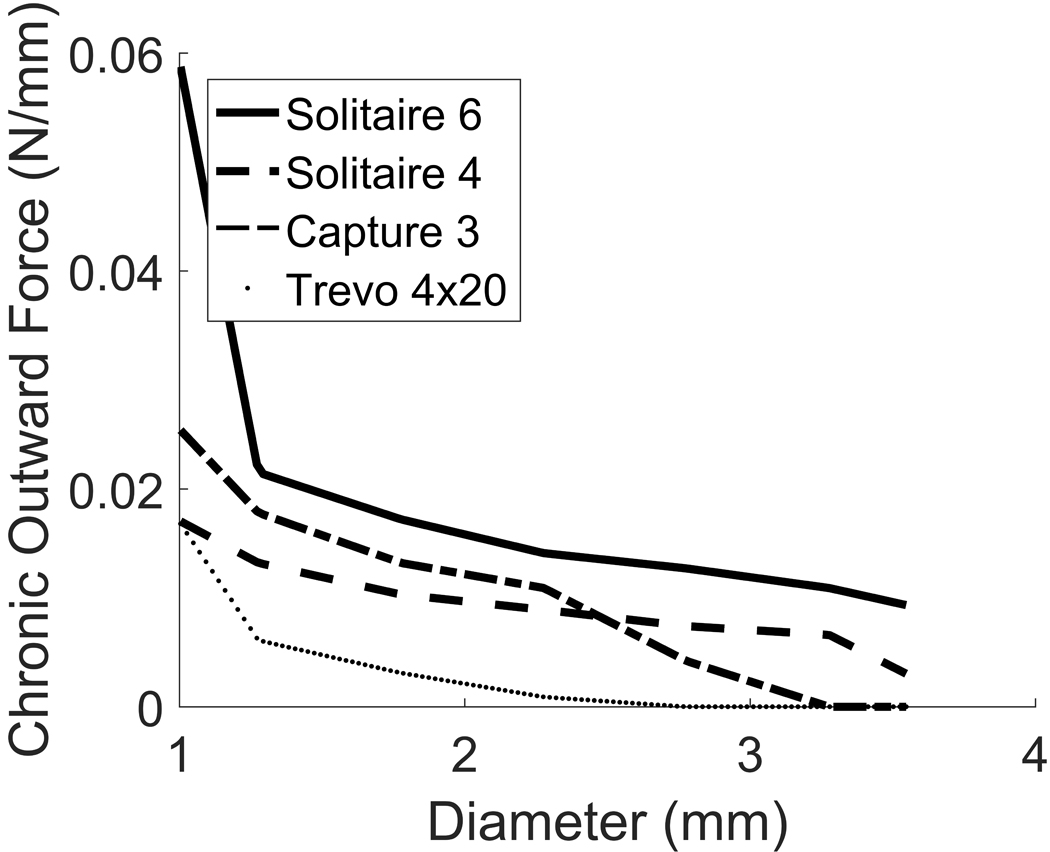
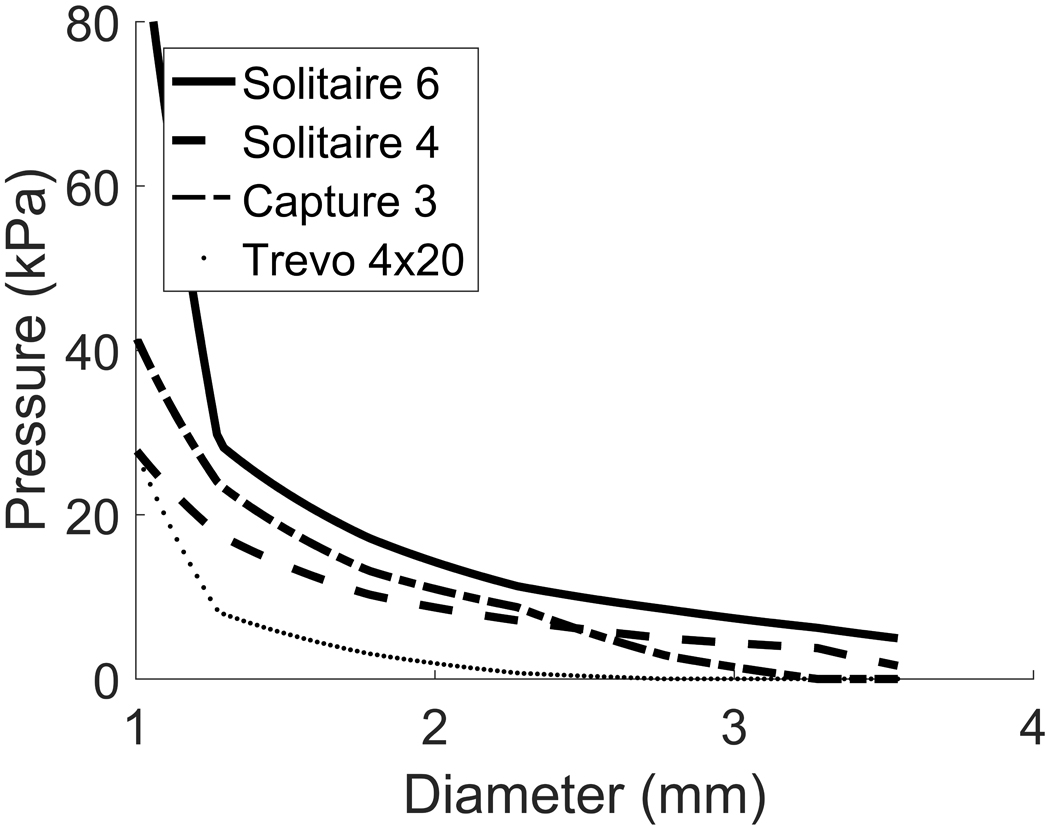
Material and methods: The arterial wall is modelled as a cylindrical membrane using a constrained mixture theory that accounts for the mechanical roles of elastin, collagen and vascular smooth muscle cells (VSMC). We model the pressure diameter curve prior to CVS and predict how it changes following CVS. We propose a stretch-based damage criterion for VSMC and evaluate if several commercially available stents are able to resolve vasospasm.
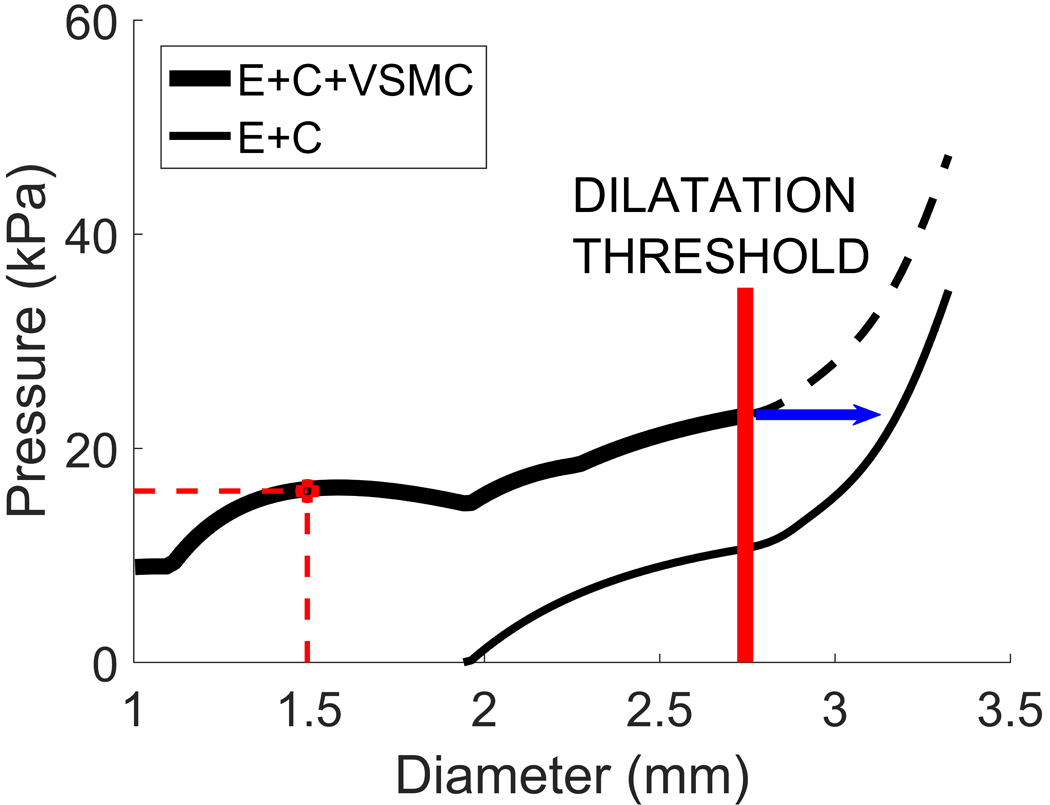
Results: The model predicts that dilatation of VSMCs beyond a threshold of mechanical failure is sufficient to resolve CVS without damage to the underlying extracellular matrix. Consistent with recent clinical observations, our model predicts that existing stents have the potential to provide sufficient outward force to successfully treat CVS and that success will be dependent on an appropriate match between stent and vessel.
Conclusion: Mathematical models of CVS can provide insights into biological mechanisms and explore treatment approaches. Improved understanding of the underlying mechanistic processes governing CVS and its mechanical treatment may assist in the development of dedicated stents.
Keywords: Mathematical modeling; Stent; Stentplasty; Vascular smooth muscle cells; Vasospasm.
Figures
References
-
- Honma Y, Fujiwara T, Irie K, Ohkawa M, Nagao S. Morphological changes in human cerebral arteries after percutaneous transluminal angioplasty for vasospasm caused by subarachnoid hemorrhage. Neurosurgery. 1995;36:1073–80; discussion 1080–1081. - PubMed
-
- Yamamoto Y, Smith RR, Bernanke DH. Mechanism of action of balloon angioplasty in cerebral vasospasm. Neurosurgery. 1992;30:1–5; discussion 5–6. - PubMed
-
- Kobayashi H, Ide H, Aradachi H, Arai Y, Handa Y, Kubota T. Histological studies of intracranial vessels in primates following transluminal angioplasty for vasospasm. J Neurosurg. 1993;78:481–6. - PubMed
-
- Macdonald RL, Wallace MC, Montanera WJ, Glen JA. Pathological effects of angioplasty on vasospastic carotid arteries in a rabbit model. J Neurosurg. 1995;83:111–7. - PubMed
-
- Chan PD, Findlay JM, Vollrath B, Cook DA, Grace M, Chen MH, et al. Pharmacological and morphological effects of in vitro transluminal balloon angioplasty on normal and vasospastic canine basilar arteries. J Neurosurg. 1995;83:522–30. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
