

Use of Combat Casualty Care Data to Assess the US Military Trauma System During the Afghanistan and Iraq Conflicts, 2001-2017
- PMID: 30916730
- PMCID: PMC6583837
- DOI: 10.1001/jamasurg.2019.0151
Use of Combat Casualty Care Data to Assess the US Military Trauma System During the Afghanistan and Iraq Conflicts, 2001-2017
Erratum in
-
Surname Update in Byline and Author Contributions.JAMA Surg. 2019 Jul 1;154(7):676. doi: 10.1001/jamasurg.2019.1256. JAMA Surg. 2019. PMID: 31042287 Free PMC article. No abstract available.
Abstract
Importance: Although the Afghanistan and Iraq conflicts have the lowest US case-fatality rates in history, no comprehensive assessment of combat casualty care statistics, major interventions, or risk factors has been reported to date after 16 years of conflict.
Objectives: To analyze trends in overall combat casualty statistics, to assess aggregate measures of injury and interventions, and to simulate how mortality rates would have changed had the interventions not occurred.
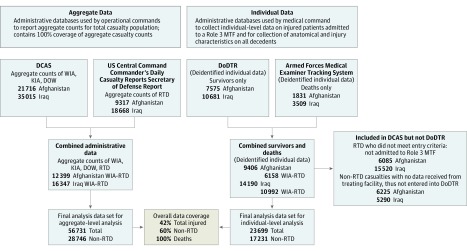
Design, setting, and participants: Retrospective analysis of all available aggregate and weighted individual administrative data compiled from Department of Defense databases on all 56 763 US military casualties injured in battle in Afghanistan and Iraq from October 1, 2001, through December 31, 2017. Casualty outcomes were compared with period-specific ratios of the use of tourniquets, blood transfusions, and transport to a surgical facility within 60 minutes.
Main outcomes and measures: Main outcomes were casualty status (alive, killed in action [KIA], or died of wounds [DOW]) and the case-fatality rate (CFR). Regression, simulation, and decomposition analyses were used to assess associations between covariates, interventions, and individual casualty status; estimate casualty transitions (KIA to DOW, KIA to alive, and DOW to alive); and estimate the contribution of interventions to changes in CFR.
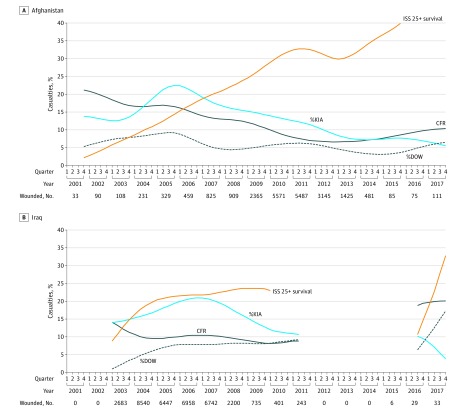
Results: In aggregate data for 56 763 casualties, CFR decreased in Afghanistan (20.0% to 8.6%) and Iraq (20.4% to 10.1%) from early stages to later stages of the conflicts. Survival for critically injured casualties (Injury Severity Score, 25-75 [critical]) increased from 2.2% to 39.9% in Afghanistan and from 8.9% to 32.9% in Iraq. Simulations using data from 23 699 individual casualties showed that without interventions assessed, CFR would likely have been higher in Afghanistan (15.6% estimated vs 8.6% observed) and Iraq (16.3% estimated vs 10.1% observed), equating to 3672 additional deaths (95% CI, 3209-4244 deaths), of which 1623 (44.2%) were associated with the interventions studied: 474 deaths (12.9%) (95% CI, 439-510) associated with the use of tourniquets, 873 (23.8%) (95% CI, 840-910) with blood transfusion, and 275 (7.5%) (95% CI, 259-292) with prehospital transport times.
Conclusions and relevance: Our analysis suggests that increased use of tourniquets, blood transfusions, and more rapid prehospital transport were associated with 44.2% of total mortality reduction. More critically injured casualties reached surgical care, with increased survival, implying improvements in prehospital and hospital care.
Conflict of interest statement
Figures
Comment in
-
Hard-earned Lifesaving Lessons From the Combat Zone.JAMA Surg. 2019 Jul 1;154(7):609. doi: 10.1001/jamasurg.2019.0152. JAMA Surg. 2019. PMID: 30916739 No abstract available.
References
-
- Rosenfeld L. Four Centuries of Clinical Chemistry. New York, NY: Taylor & Francis; 1999.
-
- Schwartz AM. The historical development of methods of hemostasis. Surgery. 1958;44(3):604-610. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
