

Time to epinephrine treatment is associated with the risk of mortality in children who achieve sustained ROSC after traumatic out-of-hospital cardiac arrest
- PMID: 30917838
- PMCID: PMC6437972
- DOI: 10.1186/s13054-019-2391-z
Time to epinephrine treatment is associated with the risk of mortality in children who achieve sustained ROSC after traumatic out-of-hospital cardiac arrest
Abstract
Background: The benefits of early epinephrine administration in pediatric with nontraumatic out-of-hospital cardiac arrest (OHCA) have been reported; however, the effects in pediatric cases of traumatic OHCA are unclear. Since the volume-related pharmacokinetics of early epinephrine may differ obviously with and without hemorrhagic shock (HS), beneficial or harmful effects of nonselective epinephrine stimulation (alpha and beta agonists) may also be enhanced with early administration. In this study, we aimed to analyze the therapeutic effect of early epinephrine administration in pediatric cases of HS and non-HS traumatic OHCA.
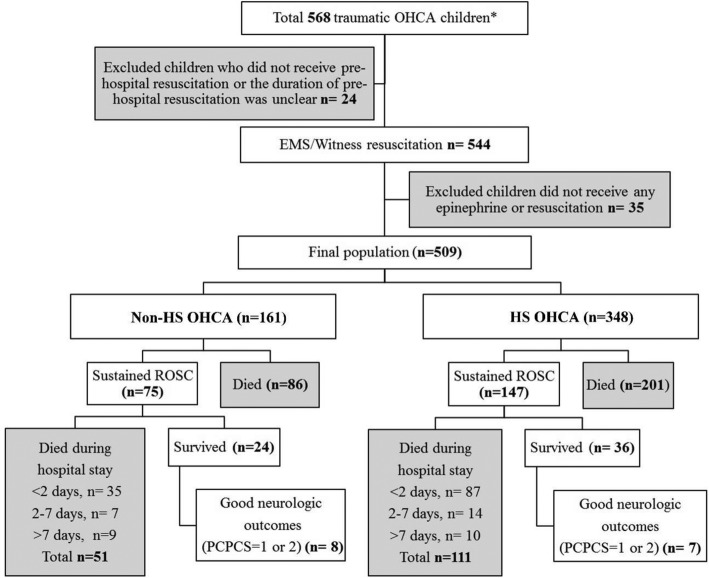
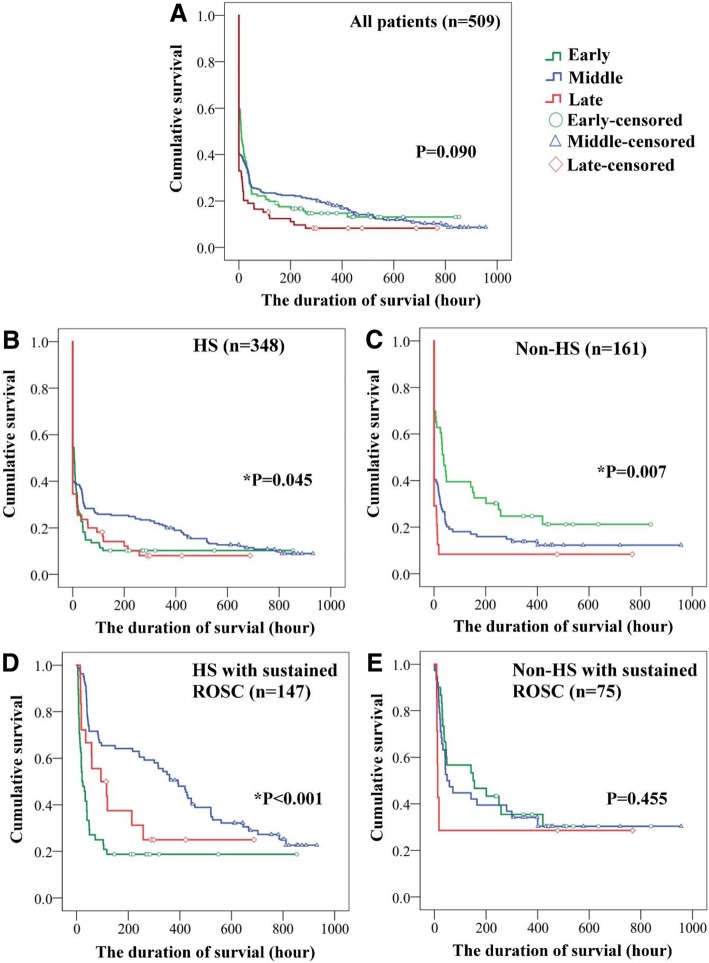
Methods: This was a multicenter retrospective study (2003-2014). Children (aged ≤ 19 years) who experienced traumatic OHCA and were administered epinephrine for resuscitation were included. Children were classified into the HS (blood loss > 30% of total body fluid) and non-HS groups. The demographics, outcomes, postresuscitation hemodynamics (the first hour) after the sustained return of spontaneous circulation (ROSC), and survival durations were analyzed and correlated with the time to epinephrine administration (early < 15, middle 15-30, late > 30 min) in the HS and non-HS groups. Cox regression analysis was used to adjust for risk factors of mortality.
Results: A total of 509 children were included. Most of them (n = 348, 68.4%) had HS OHCA. Early epinephrine administration was implemented in 131 (25.7%) children. In both the HS and non-HS groups, early epinephrine administration was associated with achieving sustained ROSC (both p < 0.05) but was not related to survival or good neurological outcomes (without adjusting for confounding factors). However, early epinephrine administration in the HS group increased cardiac output but induced metabolic acidosis and decreased urine output during the initial postresuscitation period (all p < 0.05). After adjusting for confounding factors, early epinephrine administration was a risk factor of mortality in the HS group (HR 4.52, 95% CI 2.73-15.91).
Conclusion: Early epinephrine was significantly associated with achieving sustained ROSC in pediatric cases of HS and non-HS traumatic OHCA. For children with HS, early epinephrine administration was associated with both beneficial (increased cardiac output) and harmful effects (decreased urine output and metabolic acidosis) during the postresuscitation period. More importantly, early epinephrine was a risk factor associated with mortality in the HS group.
Keywords: Children; Epinephrine; OHCA; Survival; Traumatic.
Conflict of interest statement
Ethics approval and consent to participate
This study was performed with the permission of the IRB of one medical center in central Taiwan. All review work was performed by ED physicians using a standardized abstraction form. The quality of the review was monitored by regular meetings, and the final output data were deidentified.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Comment upon "Time to epinephrine treatment is associated with the risk of mortality in children who achieve sustained ROSC after traumatic out-of-hospital cardiac arrest".Crit Care. 2019 Oct 29;23(1):336. doi: 10.1186/s13054-019-2614-3. Crit Care. 2019. PMID: 31665068 Free PMC article. No abstract available.
References
-
- Tomio J, Nakahara S, Takahashi H, Ichikawa M, Nishida M, Morimura N, Sakamoto T. Effectiveness of prehospital epinephrine administration in improving long-term outcomes of witnessed out-of-hospital cardiac arrest patients with initial non-shockable rhythms. Prehosp Emerg Care. 2017;21(4):432–441. doi: 10.1080/10903127.2016.1274347. - DOI - PubMed
-
- Perkins GD, Ji C, Deakin CD, Quinn T, Nolan JP, Scomparin C, Regan S, Long J, Slowther A, Pocock H, Black JJM, Moore F, Fothergill RT, Rees N, O'Shea L, Docherty M, Gunson I, Han K, Charlton K, Finn J, Petrou S, Stallard N, Gates S, Lall R, PARAMEDIC2 Collaborators A randomized trial of epinephrine in out-of-hospital cardiac arrest. N Engl J Med. 2018;379(8):711–721. doi: 10.1056/NEJMoa1806842. - DOI - PubMed
-
- Hansen M, Schmicker RH, Newgard CD, Grunau B, Scheuermeyer F, Cheskes S, Vithalani V, Alnaji F, Rea T, Idris AH, Herren H, Hutchison J, Austin M, Egan D, Daya M, Resuscitation outcomes consortium investigators Time to epinephrine administration and survival from nonshockable out-of-hospital cardiac arrest among children and adults. Circulation. 2018;137(19):2032–2040. doi: 10.1161/CIRCULATIONAHA.117.033067. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
