

Segment Occlusion vs. Reconstruction-A Single Center Experience With Endovascular Strategies for Ruptured Vertebrobasilar Dissecting Aneurysms
- PMID: 30918497
- PMCID: PMC6424888
- DOI: 10.3389/fneur.2019.00207
Segment Occlusion vs. Reconstruction-A Single Center Experience With Endovascular Strategies for Ruptured Vertebrobasilar Dissecting Aneurysms
Abstract
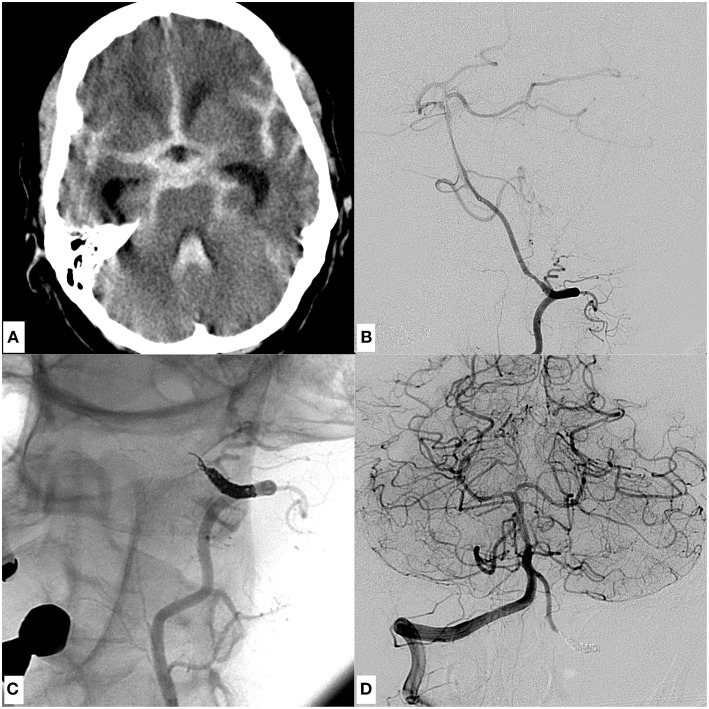
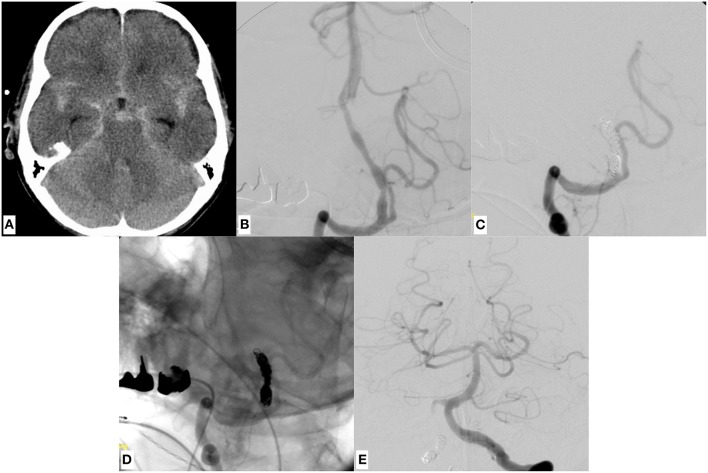
Objective: Ruptured dissecting aneurysms of the intracranial vertebral arteries exhibit an extraordinarily high risk for morbidity and mortality and are prone to re-rupture. Therefore, early treatment is mandatory to induce stagnation of the critical dynamic mural process. Appropriate endovascular approaches are segment sacrifice and reconstruction, however, both carry specific risks and benefits. To date most studies discuss only one of these approaches and focus on one specific device or technique. Therefore, our study aimed to present our experiences with both techniques, providing a considered approach on when to perform endovascular reconstruction or sacrifice. Materials and Methods: We retrospectively reviewed patients with subarachnoid hemorrhage in our database, suffering from dissecting aneurysms of the intradural vertebral arteries and treated endovascularly in the acute setting. A total of 16 cases were included. Clinical history, radiologic findings and outcomes were analyzed. Results: In 7 patients a reconstructive approach was chosen with 4 of them receiving stent-assisted coiling as primary strategy. One of the 7 patients suffered early re-bleeding due to progression of the dissection and therefore treatment was augmented with implantation of 2 flow diverters. The remaining 2 patients were primarily treated with flow diverters in telescoping technique. In 9 patients a deconstructive approach was followed: 6 patients were treated with proximal coil-occlusion of the V4 segment, 3 patients received distal coiling of the V4 segment. Two patients died (GOS 1) in the subacute stage due to sequelae of recurrent episodes of raised intracranial pressure and parenchymal hemorrhage. Two patients kept severe disability (GOS 3), six patients had moderate disability (GOS 4) and seven patients showed full recovery (GOS 5). None of the patients suffered from a procedural or postprocedural ischemic stroke. Conclusions: In patients with good collateral vascularization, proximal, or distal partial segment sacrifice via with endovascular coil occlusion seems to yield the best risk-benefit ratio for treatment of ruptured dissecting V4 aneurysms, especially since no continued anticoagulation is required and possibly essential surgery remains feasible in this scenario. If possible, PICA occlusion should be avoided-although even proximal PICA occlusion can become necessary, when weighing against the risk of an otherwise untreated ruptured V4 dissecting aneurysm. Contrarily, if the dominant V4 segment is affected, the hemodynamic asymmetry prohibits occlusion and necessitates reconstruction of the respective segment. For this, implants with high metal coverage treating the entire affected segment appear to be the most promising approach.
Keywords: dissecting aneurysm; flow diverter; segment occlusion; stent assisted coiling; subarachnoid hemorrhage; vertebral artery.
Figures





References
-
- Yamada M, Miyasaka Y, Yagishita S, Fujii K. Dissecting aneurysm of the intracranial vertebral artery associated with proximal focal degeneration of the elastica: a comparative pathological study of the vertebral artery in patients with and without aneurysms. Surg Neurol. (2003) 60:431–7; discussion 437. 10.1016/S0090-3019(03)00324-0 - DOI - PubMed
-
- Boström K, Liliequist B. Primary dissecting aneurysm of the extracranial part of the internal carotid and vertebral arteries. A report of three cases. Neurology. (1967) 17:179–86. - PubMed
LinkOut - more resources
Full Text Sources