

Cancer- and Chemotherapy-Induced Musculoskeletal Degradation
- PMID: 30918923
- PMCID: PMC6419610
- DOI: 10.1002/jbm4.10187
Cancer- and Chemotherapy-Induced Musculoskeletal Degradation
Abstract
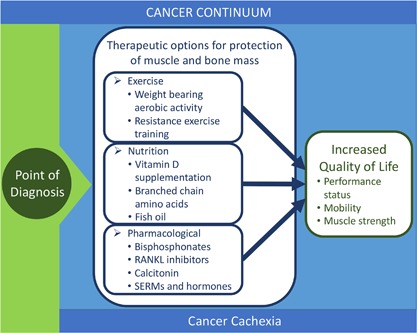
Mobility in advanced cancer patients is a major health care concern and is often lost in advanced metastatic cancers. Erosion of mobility is a major component in determining quality of life but also starts a process of loss of muscle and bone mass that further devastates patients. In addition, treatment options become limited in these advanced cancer patients. Loss of bone and muscle occurs concomitantly. Advanced cancers that are metastatic to bone often lead to bone loss (osteolytic lesions) but may also lead to abnormal deposition of new bone (osteoblastic lesions). However, in both cases there is a disruption to normal bone remodeling and radiologic evidence of bone loss. Many antitumor therapies can also lead to loss of bone in cancer survivors. Bone loss releases cytokines (TGFβ) stored in the mineralized matrix that can act on skeletal muscle and lead to weakness. Likewise, loss of skeletal muscle mass leads to reduced bone mass and quality via mechanical and endocrine signals. Collectively these interactions are termed bone-muscle cross-talk, which has garnered much attention recently as a prime target for musculoskeletal health. Pharmacological approaches as well as nutrition and exercise can improve muscle and bone but have fallen short in the context of advanced cancers and cachexia. This review highlights our current knowledge of these interventions and discusses the difficulties in treating severe musculoskeletal deficits with the emphasis on improving not only bone mass and muscle size but also functional outcomes. © 2019 The Authors. JBMR Plus published by Wiley Periodicals, Inc. on behalf of American Society for Bone and Mineral Research.
Keywords: BONE‐MUSCLE INTERACTIONS; CANCER; CHEMOTHERAPY; TUMOR‐INDUCED BONE DISEASE.
Figures
Similar articles
-
Chemotherapy-induced loss of bone and muscle mass in a mouse model of breast cancer bone metastases and cachexia.JCSM Rapid Commun. 2019 Jan-Jun;2(1):e00075. JCSM Rapid Commun. 2019. PMID: 31032492 Free PMC article.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Molecular mechanisms of bone metastasis and associated muscle weakness.Clin Cancer Res. 2014 Jun 15;20(12):3071-7. doi: 10.1158/1078-0432.CCR-13-1590. Epub 2014 Mar 27. Clin Cancer Res. 2014. PMID: 24677373 Free PMC article. Review.
-
Bone-Muscle Crosstalk: Musculoskeletal Complications of Chemotherapy.Curr Osteoporos Rep. 2022 Dec;20(6):433-441. doi: 10.1007/s11914-022-00749-4. Epub 2022 Sep 10. Curr Osteoporos Rep. 2022. PMID: 36087213 Review.
-
Biomechanical Stimulation of Muscle Constructs Influences Phenotype of Bone Constructs by Modulating Myokine Secretion.JBMR Plus. 2023 Aug 15;7(11):e10804. doi: 10.1002/jbm4.10804. eCollection 2023 Nov. JBMR Plus. 2023. PMID: 38025033 Free PMC article.
Cited by
-
Alterations in Muscle Architecture: A Review of the Relevance to Individuals After Limb Salvage Surgery for Bone Sarcoma.Front Pediatr. 2020 Jun 16;8:292. doi: 10.3389/fped.2020.00292. eCollection 2020. Front Pediatr. 2020. PMID: 32612962 Free PMC article.
-
Case report: Chest radiotherapy-induced vertebral fractures in lung cancer patients: a case series and literature review.Front Oncol. 2025 Feb 3;15:1438120. doi: 10.3389/fonc.2025.1438120. eCollection 2025. Front Oncol. 2025. PMID: 39963102 Free PMC article.
-
Changes in sagittal spinopelvic alignment are associated with increased pain and impaired function in multiple myeloma patients.Eur Spine J. 2025 Apr 26. doi: 10.1007/s00586-025-08878-x. Online ahead of print. Eur Spine J. 2025. PMID: 40285842
-
The Effect of Mild Exercise in the Chemotherapy Room on the Anxiety Level of Cancer Patients: A Prospective Observational Paired Cohort Study.J Clin Med. 2025 Aug 7;14(15):5591. doi: 10.3390/jcm14155591. J Clin Med. 2025. PMID: 40807210 Free PMC article.
-
Chemotherapy agents reduce protein synthesis and ribosomal capacity in myotubes independent of oxidative stress.Am J Physiol Cell Physiol. 2021 Dec 1;321(6):C1000-C1009. doi: 10.1152/ajpcell.00116.2021. Epub 2021 Oct 27. Am J Physiol Cell Physiol. 2021. PMID: 34705587 Free PMC article.
References
-
- Fang J, Xu Q. Differences of osteoblastic bone metastases and osteolytic bone metastases in clinical features and molecular characteristics. Clin Transl Oncol. 2015;17:173–9. - PubMed
-
- Liede A, Jerzak KJ, Hernandez RK, Wade SW, Sun P, Narod SA. The incidence of bone metastasis after early‐stage breast cancer in Canada. Breast Cancer Res Treat. 2016;156:587–95. - PubMed
-
- Joniau S, Briganti A, Gontero P, et al. Stratification of high‐risk prostate cancer into prognostic categories: a European multi‐institutional study. Eur Urol. 2015;67:157–64. - PubMed
-
- Oliveira MB, Mello FC, Paschoal ME. The relationship between lung cancer histology and the clinicopathological characteristics of bone metastases. Lung Cancer. 2016;96:19–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources