

Treatment of cancer-associated venous thromboembolism in the age of direct oral anticoagulants
- PMID: 30918939
- PMCID: PMC6594460
- DOI: 10.1093/annonc/mdz111
Treatment of cancer-associated venous thromboembolism in the age of direct oral anticoagulants
Abstract
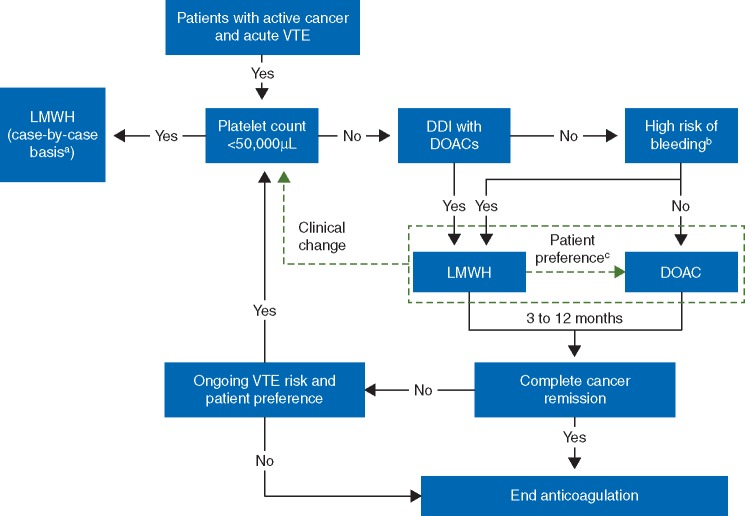
Anticoagulation for cancer-associated venous thromboembolism (VTE) can be challenging due to complications-including bleeding and potential drug-drug interactions with chemotherapy-associated with vitamin K antagonists and inconvenience of low-molecular-weight heparin (LMWH). Direct oral anticoagulants (DOACs) could partially overcome these issues, but until recently there were no large clinical trials assessing their efficacy and safety in cancer patients. This review summarizes clinical treatment guidelines, prior clinical and real-world evidence for anticoagulant choice, recent clinical trials assessing DOACs for cancer-associated VTE (i.e. Hokusai-VTE Cancer, SELECT-D, CARAVAGGIO, and ADAM VTE), and special considerations for DOAC use. Based on established data, clinical guidelines recommend patients with cancer-associated VTE receive LMWH treatment of at least 3-6 months. Nevertheless, LMWH is underused and associated with poor compliance and persistence in these patients relative to oral anticoagulants. Clinical data supporting DOAC use in cancer patients are becoming available. In Hokusai-VTE Cancer, edoxaban was noninferior to dalteparin for the composite of recurrent VTE and major bleeding (12.8% versus 13.5%), with numerically lower recurrent VTE (7.9% versus 11.3%) and significantly higher major bleeding (6.9% versus 4.0%); only patients with gastrointestinal cancer had significantly higher risk of bleeding with edoxaban. In SELECT-D, rivaroxaban had numerically lower VTE recurrence (4% versus 11%), comparable major bleeding (6% versus 4%), and numerically higher clinically relevant nonmajor bleeding (13% versus 4%) versus dalteparin. Most bleeding events were gastrointestinal or urologic; patients with esophageal/gastroesophageal cancer had higher rates of major bleeding with rivaroxaban (36% versus 11%). For comparison of apixaban versus dalteparin, CARAVAGGIO is ongoing, and preliminary results from ADAM VTE are favorable. This review concludes that DOACs appear to be reasonable alternatives to LMWH for treatment of cancer-associated VTE. In patients with gastrointestinal cancer, DOAC use should be considered on a case-by-case basis with consideration of the relative risks and benefits.
Keywords: cancer; direct oral anticoagulants; treatment; venous thromboembolism.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
Figures
Comment in
-
Interactions between direct anticoagulants and chemotherapy.Ann Oncol. 2019 Jul 1;30(7):1170. doi: 10.1093/annonc/mdz137. Ann Oncol. 2019. PMID: 31046105 Free PMC article. No abstract available.
References
-
- Chew HK, Wun T, Harvey D. et al. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med 2006; 166(4): 458–464. - PubMed
-
- Khorana AA, Francis CW, Culakova E. et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost 2007; 5(3): 632–634. - PubMed
-
- Merkow RP, Bilimoria KY, Tomlinson JS. et al. Postoperative complications reduce adjuvant chemotherapy use in resectable pancreatic cancer. Ann Surg 2014; 260(2): 372–377. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
