

Canagliflozin Prevents Intrarenal Angiotensinogen Augmentation and Mitigates Kidney Injury and Hypertension in Mouse Model of Type 2 Diabetes Mellitus
- PMID: 30921791
- PMCID: PMC6475450
- DOI: 10.1159/000499597
Canagliflozin Prevents Intrarenal Angiotensinogen Augmentation and Mitigates Kidney Injury and Hypertension in Mouse Model of Type 2 Diabetes Mellitus
Abstract
Background: Hypertension and renal injury are common complications of type 2 diabetes mellitus (T2DM). Hyperglycemia stimulates renal proximal tubular angiotensinogen (AGT) expression via elevated oxidative stress contributing to the development of high blood pressure and diabetic nephropathy. The sodium glucose cotransporter 2 (SGLT2) in proximal tubules is responsible for the majority of glucose reabsorption by renal tubules. We tested the hypothesis that SGLT2 inhibition with canagliflozin (CANA) prevents intrarenal AGT augmentation and ameliorates kidney injury and hypertension in T2DM.
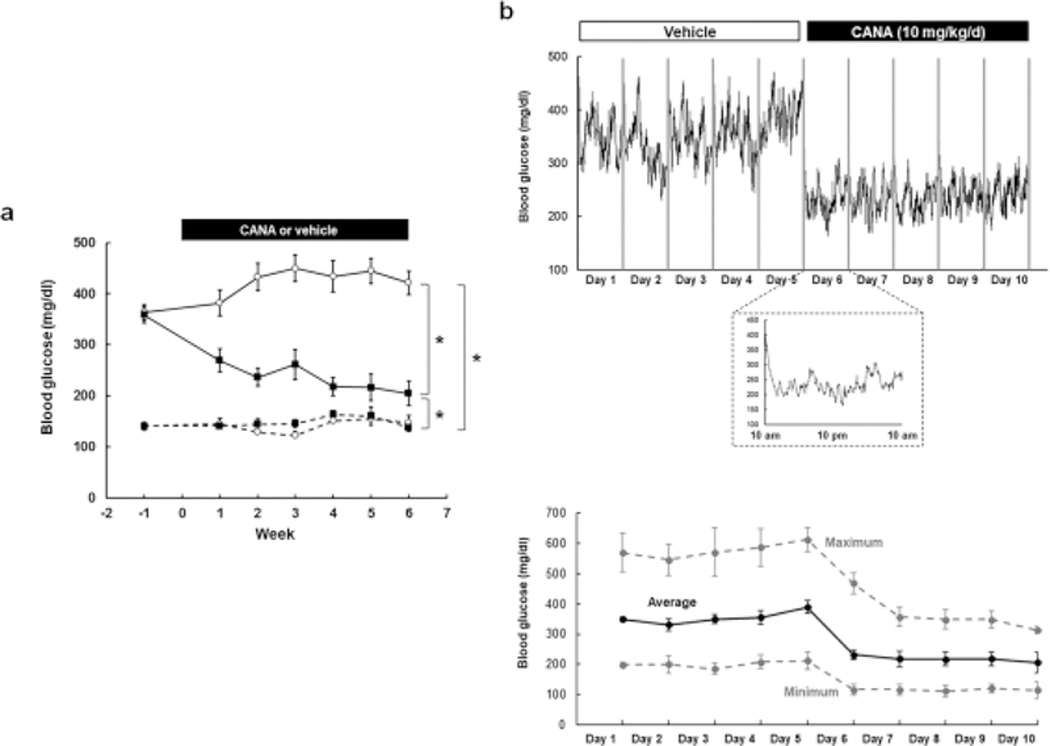
Methods: We induced T2DM in New Zealand obese mice with a high fat diet (DM, 30% fat) with control mice receiving regular fat diet (ND, 4% fat). When DM mice exhibited > 350 mg/dL blood glucose levels, both DM- and ND-fed mice were treated with 10 mg/kg/day CANA or vehicle by oral gavage for 6 weeks. We evaluated intrarenal AGT, blood pressure, and the development of kidney injury.
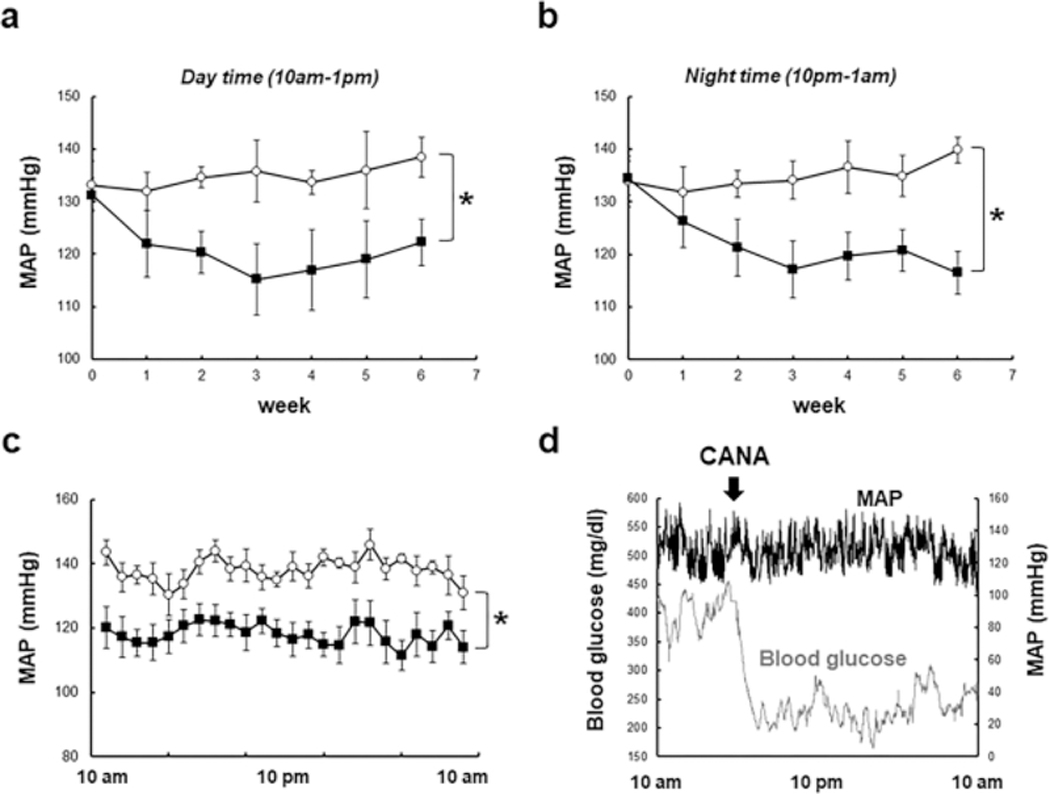
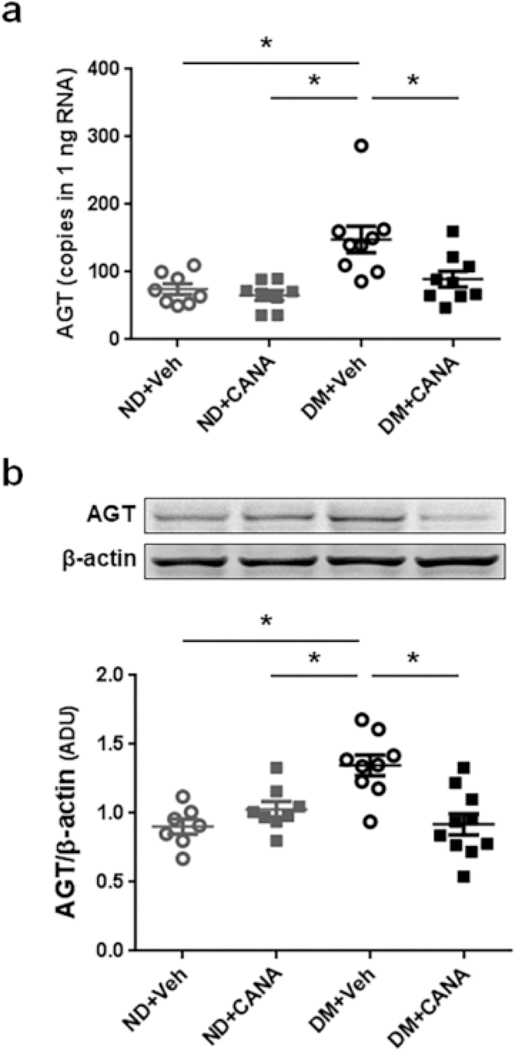
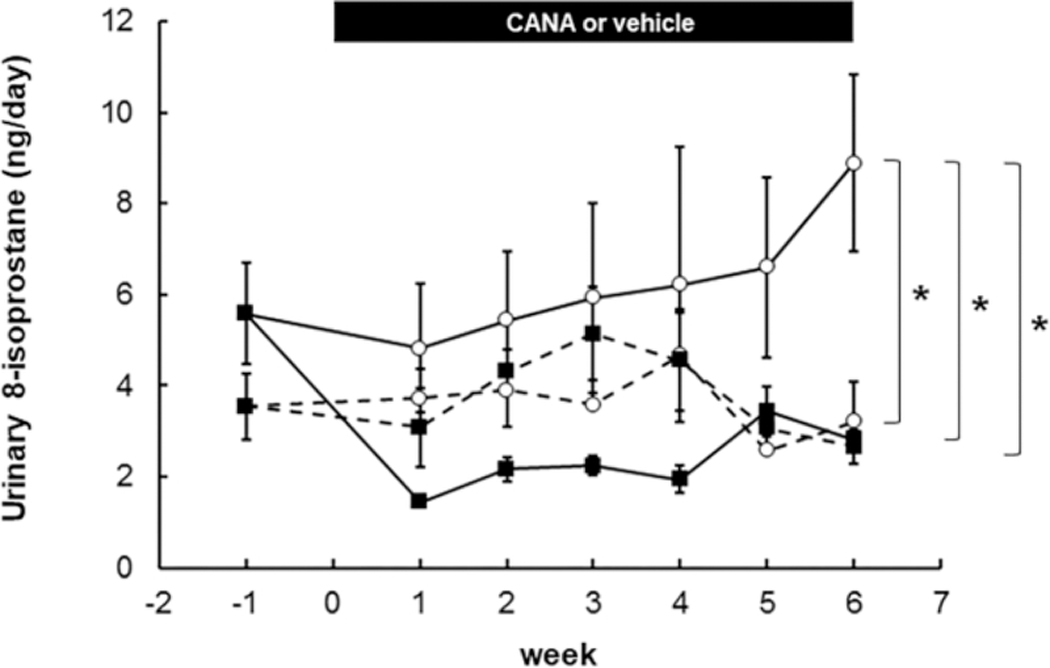
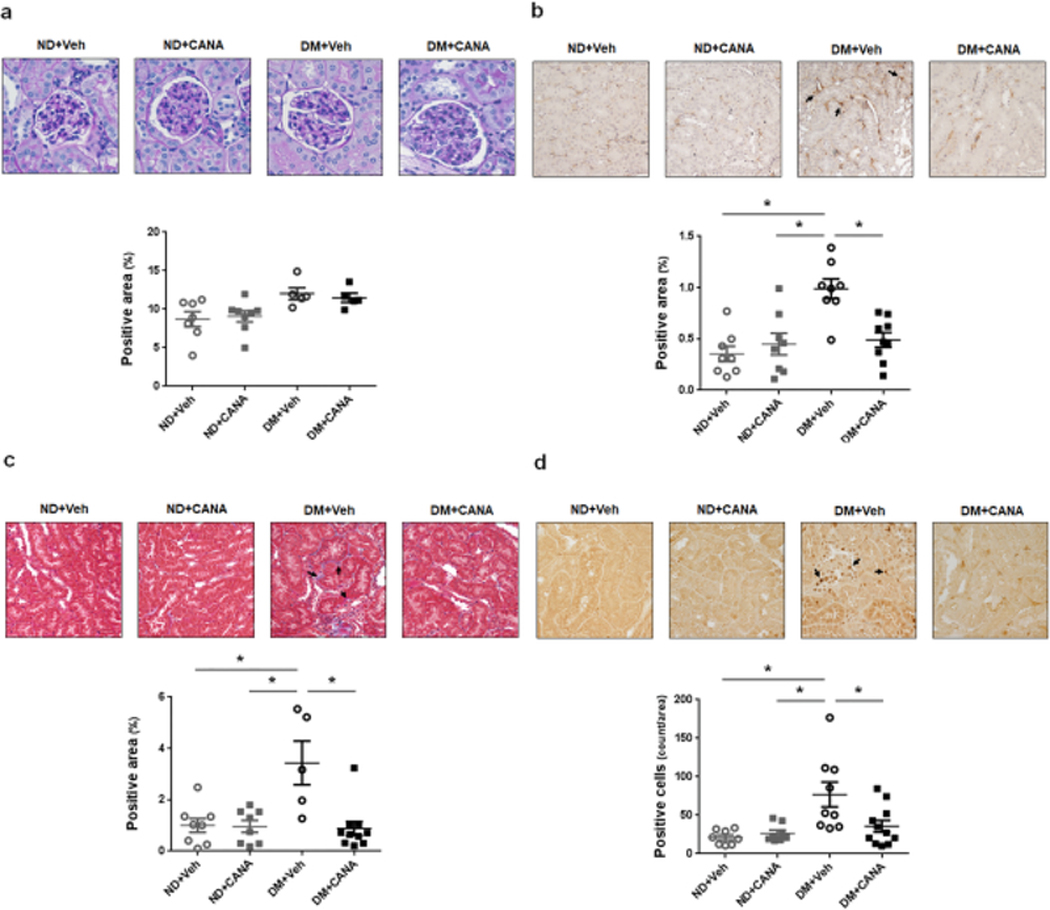
Results: Systolic blood pressure in DM mice (133.9 ± 2.0 mm Hg) was normalized by CANA (113.9 ± 4.0 mm Hg). CANA treatment ameliorated hyperglycemia-associated augmentation of renal AGT mRNA (148 ± 21 copies/ng RNA in DM, and 90 ± 16 copies/ng RNA in DM + CANA) and protein levels as well as elevation of urinary 8-isoprostane levels. Tubular fibrosis in DM mice (3.4 ± 0.9-fold, fibrotic score, ratio to ND) was suppressed by CANA (0.9 ± 0.3-fold). Furthermore, CANA attenuated DM associated increased macrophage infiltration and cell proliferation in kidneys of DM mice.
Conclusions: CANA prevents intrarenal AGT upregulation and oxidative stress and which may mitigate high blood pressure, renal tubular fibrosis, and renal inflammation in T2DM.
Keywords: Angiotensinogen; Blood pressure; Diabetes mellitus; Kidney; Sodium glucose cotransporter 2 inhibition.
© 2019 S. Karger AG, Basel.
Figures
Comment in
-
Renal Angiotensinogen and Sodium-Glucose Cotransporter-2 Inhibition: Insights from Experimental Diabetic Kidney Disease.Am J Nephrol. 2019;49(4):328-330. doi: 10.1159/000499598. Epub 2019 Mar 28. Am J Nephrol. 2019. PMID: 30921790 No abstract available.
References
-
- Kobori H, Nangaku M, Navar LG, Nishiyama A: The intrarenal renin-angiotensin system: from physiology to the pathobiology of hypertension and kidney disease. Pharmacological reviews, 59: 251–287, 2007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
