

Outcome of conservative and surgical treatment of enchondromas and atypical cartilaginous tumors of the long bones: retrospective analysis of 228 patients
- PMID: 30922289
- PMCID: PMC6440168
- DOI: 10.1186/s12891-019-2502-7
Outcome of conservative and surgical treatment of enchondromas and atypical cartilaginous tumors of the long bones: retrospective analysis of 228 patients
Abstract
Background: Sufficient data on outcome of patients with clinically and radiologically aggressive enchondromas and atypical cartilaginous tumors (ACT) is lacking. We therefore analyzed both conservatively and surgically treated patients with lesions, which were not distinguishable between benign enchondroma and low-grade malignant ACT based upon clinical and radiologic appearance.
Methods: The series included 228 consecutive cases with a follow-up > 24 months to assess radiological, histological, and clinical outcome including recurrences and complications. Pain, satisfaction, functional limitations, and the musculoskeletal tumor society (MSTS) score were evaluated to judge both function and emotional acceptance at final follow-up.
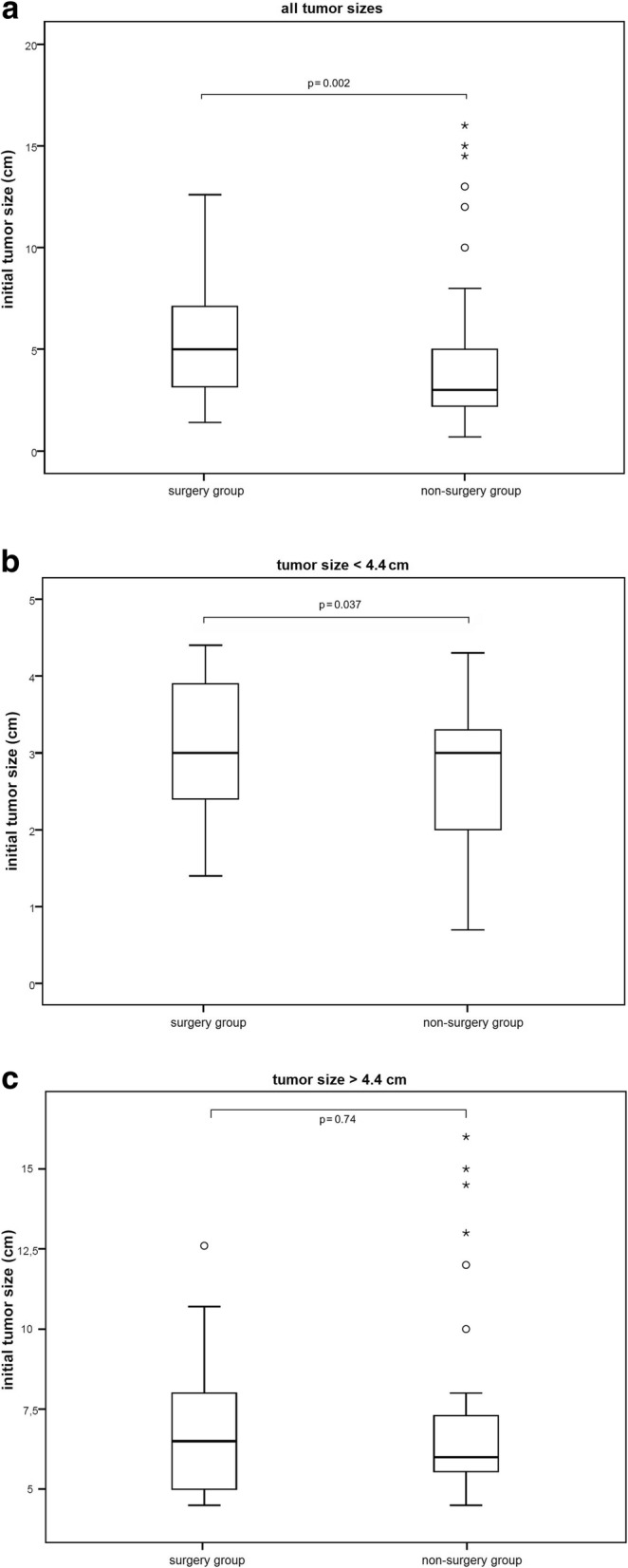
Results: Follow-up took place at a mean of 82 (median 75) months. The 228 patients all had comparable clinical and radiological findings. Of these, 153 patients were treated conservatively, while the other 75 patients underwent intralesional curettage. Besides clinical and radiological aggressiveness, most lesions were histologically judged as benign enchondromas. 9 cases were determined to be ACT, while the remaining 7 cases had indeterminate histology. After surgery, three patients developed a recurrence, and a further seven had complications of which six were related to osteosynthesis. Both groups had excellent and almost equal MSTS scores of 96 and 97%, respectively, but significantly less functional limitations were found in the non-surgery group. Further sub-analyses were performed to reduce selection bias. Sub-analysis of histologically diagnosed enchondromas in the surgery group found more pain, less function, and worse MSTS score compared to the non-surgery group. Sub-analysis of smaller lesions (< 4.4 cm) did not show significant differences. In contrast, larger lesions displayed significantly worse results after surgery compared to conservative treatment (enchondromas > 4.4 cm: MSTS score: 94.0% versus 97.3%, p = 0.007; pain 2.3 versus 0.8, p = 0.001). The majority of lesions treated surgically was filled with polymethylmethacrylate bone-cement, while the remainder was filled with cancellous-bone, without significant difference in clinical outcome.
Conclusion: Feasibility of intralesional curettage strategies for symptomatic benign to low-grade malignant chondrogenic tumors was supported. Surgery, however, did not prove superior compared to conservative clinical and radiological observation. Due to the low risk of transformation into higher-grade tumors and better functional results, more lesions might just be observed if continuous follow-up is assured.
Keywords: ACT; Bone-cement; Chondrosarcoma; Curettage; Enchondroma; Long bones.
Conflict of interest statement
Ethics approval and consent to participate
Approval was given by our ethical committee of the University of Heidelberg, Germany (votum number S-053/2017). Informed written consent was obtained from all patients. For patients younger than 18-years written consent was obtained on their behalf by a parent/legal guardian.
Consent for publication
not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
