

Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: a meta-analysis
- PMID: 30922308
- PMCID: PMC6437888
- DOI: 10.1186/s12941-019-0313-1
Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: a meta-analysis
Abstract
Background: Maternal rectovaginal colonization with Streptococcus agalactiae (Group B Streptococcus or GBS) is the most common route for the GBS disease in the perinatal period. The knowledge of maternal colonization, antibiotic resistance and serotype profiles is substantially needed to formulate the broad vaccine. However, it has not been estimated in Africa. This meta-analysis was aimed to determine the pooled prevalence of colonization, antibiotic resistance and serotype profiles of GBS reported in Africa.
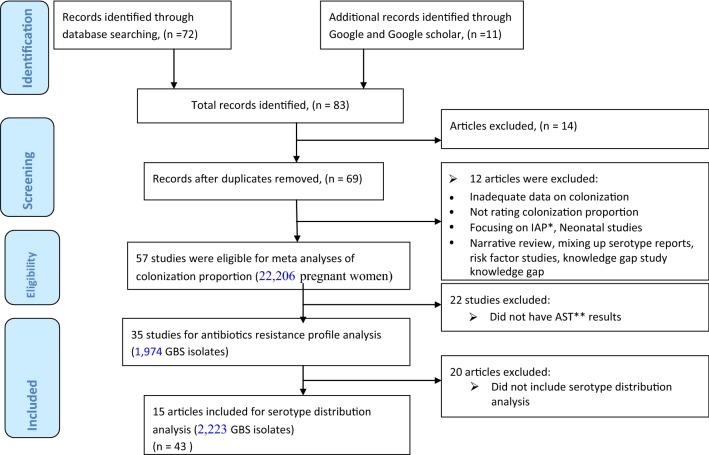
Methods: Potentially relevant studies from 1989 to 31th January, 2019 were retrieved from the Medline/PubMed, EMBASE, HINARI online databases, periodicals and by requesting authors. Unpublished studies retrieved from grey literature through Google and Google Scholar. Pooled estimates were calculated using the random effect model. Subgroup analysis was done to investigate the burden of colonization across sub-regions, sampling site and countries. Summary estimates were presented using words, Forest plots and Tables. Heterogeneity was assessed using the I2 statistic.
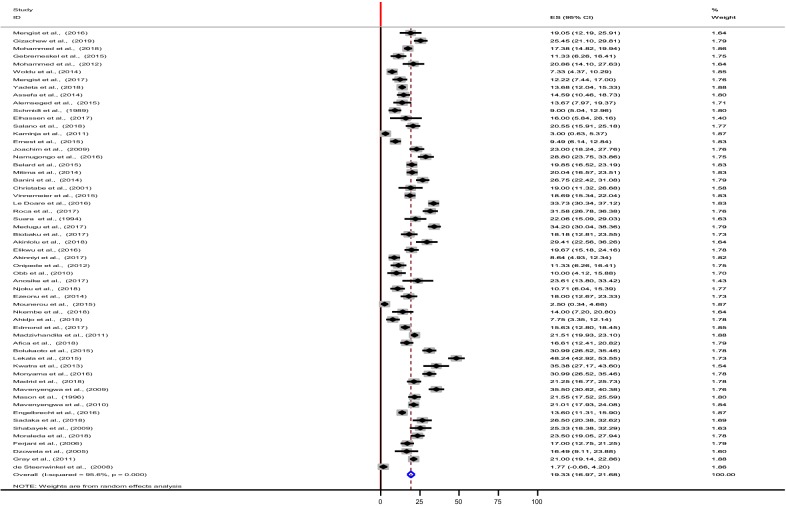
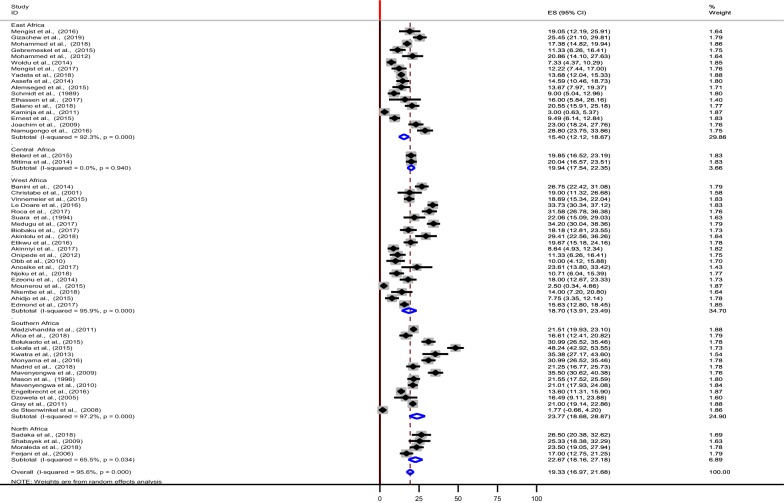
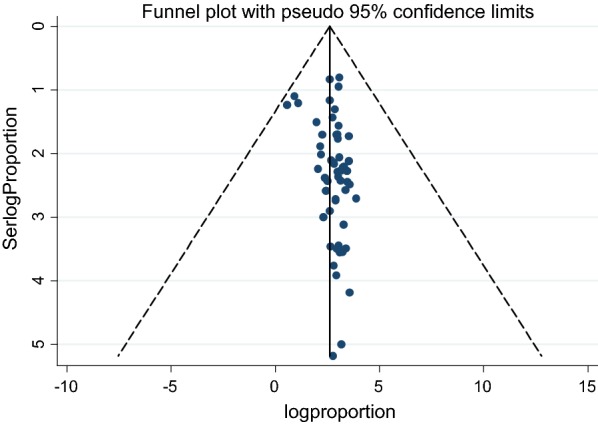
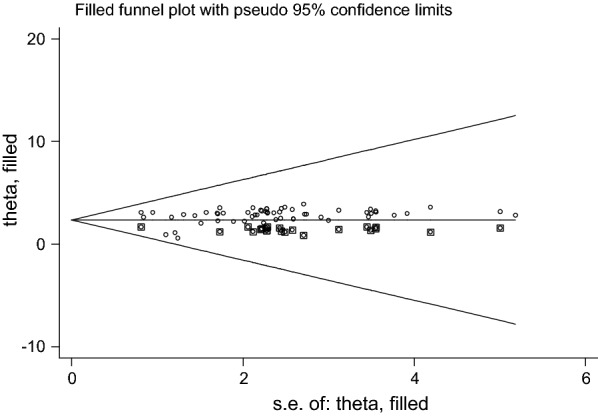
Results: Eighty-three articles were assessed, of which 57 studies conducted in five sub-regions with 21 countries (22,206 pregnant women) met pre-specified inclusion criteria. The overall estimate of recto-vaginal colonization was 19.3% (95% CI 16.9, 21.7). The highest estimate was observed in Southern Africa, 23.8% (95% CI 18.7, 28.9), followed by Northern Africa, 22.7% (95% CI 18.2, 27.2) while the lowest was driven from the Eastern Africa, 15.4% (95% CI 12.1, 18.7). Considerable heterogeneity across and within regions, sampling site, screening methods and countries (I2 > 75%); and the publication bias were observed (p = 0.031). GBS showed the highest resistance to tetracycline. Resistance to penicillin, amoxicillin, chloramphenicol, ampicillin, ceftriaxone, ciprofloxacin, erythromycin, vancomycin and clindamycin also observed. The V, III, Ia, Ib, and II serotypes altogether were accounted 91.8% in the African studies.
Conclusions: The pooled estimate of the maternal colonization with GBS was 19.3% which is equivalent with other many primary and review reports worldwide. The most antibiotic resistance estimate was recorded in the tetracycline followed by penicillin. Five serotypes were the most prevalent in Africa and more data on the antibiotic résistance and serotype distribution patterns are needed from developing countries to devise the effective preventive measures. In addition, the antibiotic susceptibility test methods used in the Africa shall be assessed for its quality. Trial registration Prospero Registration Number CRD42018094525.
Keywords: Antibiotic resistance; Colonization; GBS; Pregnant women; Recto-vaginal; Serotypes.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
-
- Sambola A, Miro JM, Tornos MP, Almirante B, Moreno-Torrico A, Gurgui M, et al. Streptococcus agalactiae infective endocarditis: analysis of 30 cases and review of the literature, 1962–1998. Clin Infect Dis. 2002;34:1576–1584. - PubMed
-
- Centers for Disease Control and Prevention Prevention of perinatal Group B Streptococcal disease: revised guidelines from CDC. MMWR Recomm Rep. 2010;59(No. RR-10):1–36. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
