

Mucinous colorectal adenocarcinoma: clinical pathology and treatment options
- PMID: 30922401
- PMCID: PMC6440160
- DOI: 10.1186/s40880-019-0361-0
Mucinous colorectal adenocarcinoma: clinical pathology and treatment options
Abstract
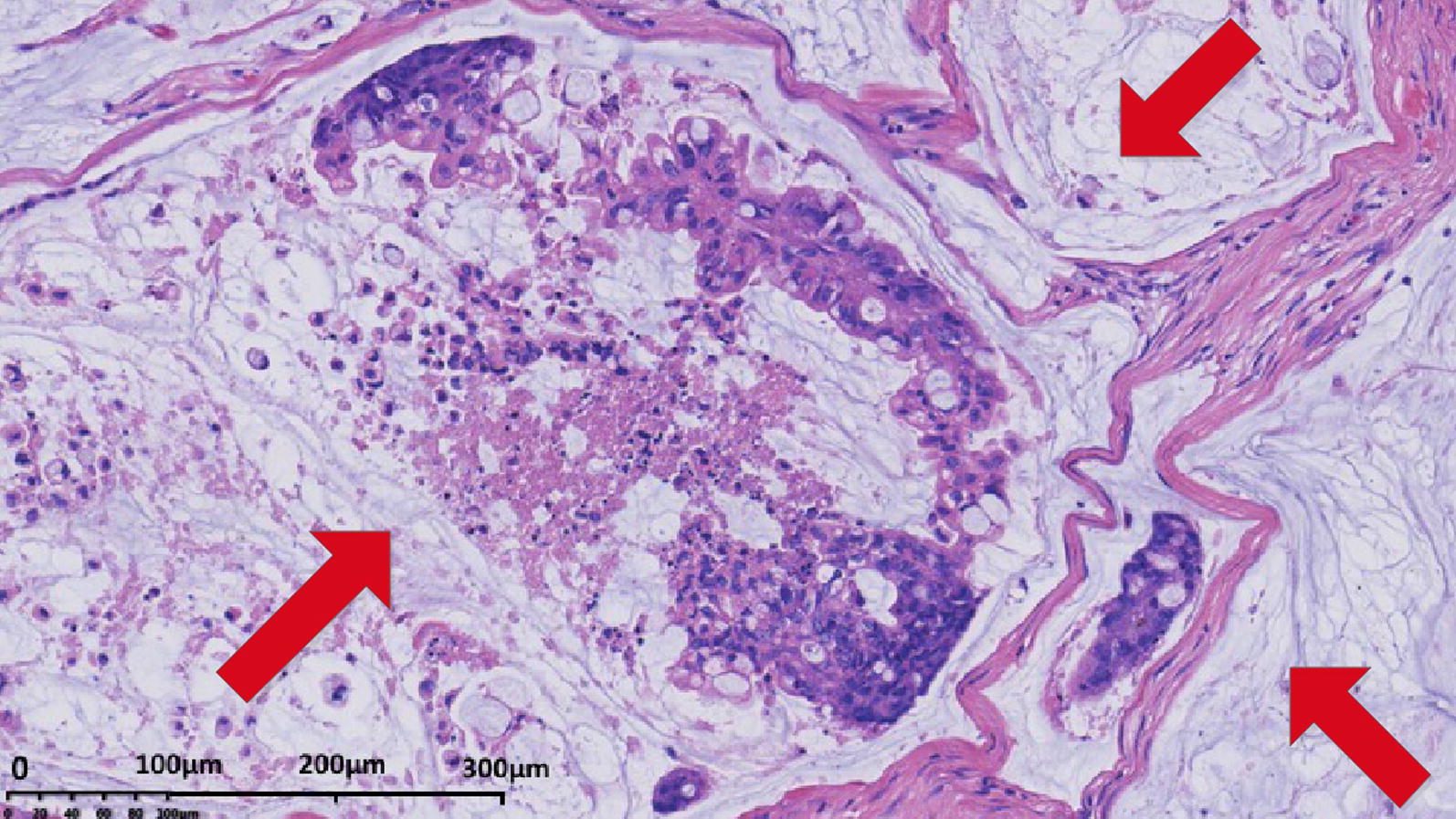
Mucinous colorectal adenocarcinoma is a distinct subtype of colorectal cancer (CRC) characterized by the presence of abundant extracellular mucin which accounts for at least 50% of the tumor volume. Mucinous colorectal adenocarcinoma is found in 10%-20% of CRC patients and occurs more commonly in female and younger patients. Moreover, mucinous colorectal adenocarcinoma is more frequently located in the proximal colon and diagnosed at an advanced stage. Based on its molecular context, mucinous colorectal adenocarcinoma is associated with the overexpression of mucin 2 (MUC2) and mucin 5AC (MUC5AC) proteins. At the same time, it shows higher mutation rates in the fundamental genes of the RAS/MAPK and PI3K/Akt/mTOR pathways. Mucinous colorectal adenocarcinoma also shows higher rates of microsatellite instability (MSI) than non-mucinous colorectal adenocarcinoma which might correlate it with Lynch syndrome and the CpG island methylator phenotype. The prognosis of mucinous colorectal adenocarcinoma as to non-mucinous colorectal adenocarcinoma is debatable. Further, the impaired responses of mucinous colorectal adenocarcinoma to palliative or adjuvant chemotherapy warrant more studies to be performed for a specialized treatment for these patients. In this review, we discuss the molecular background and histopathology of mucinous colorectal adenocarcinoma, and provide an update on its prognosis and therapeutics from recent literatures.
Keywords: Adenocarcinoma; Colorectal cancer; Hyperthermic intraperitoneal chemotherapy; Immunotherapy; Lynch syndrome; MUC2; MUC5AC; Microsatellite instability; Mucinous carcinoma; Targeted molecular therapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4. Geneva: World Health Organization Classification of Tumours; 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
