

Utility of positron emission tomography-computed tomography in patients with chronic lymphocytic leukemia following B-cell receptor pathway inhibitor therapy
- PMID: 30923097
- PMCID: PMC6821597
- DOI: 10.3324/haematol.2018.207068
Utility of positron emission tomography-computed tomography in patients with chronic lymphocytic leukemia following B-cell receptor pathway inhibitor therapy
Abstract
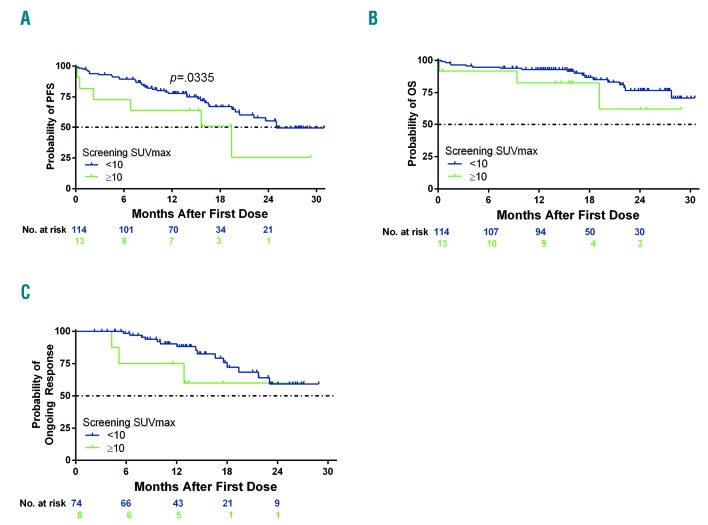
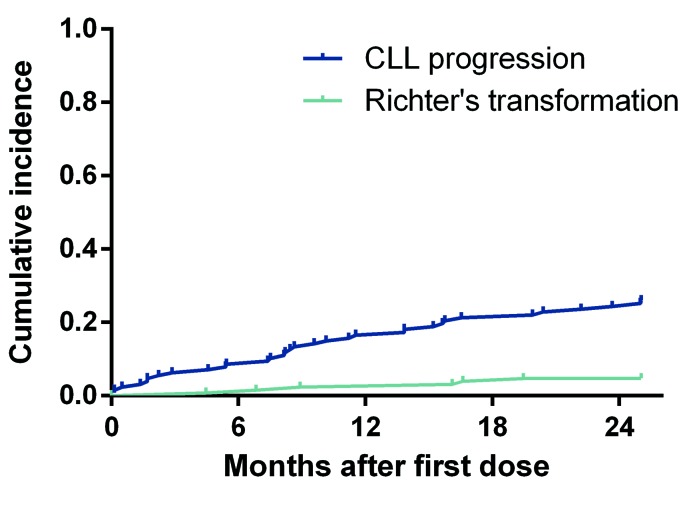
The utility of positron emission tomography-computed tomography (PET-CT) in distinguishing Richter's transformation versus chronic lymphocytic leukemia (CLL) progression after ibrutinib and/or idelalisib was assessed in a post hoc analysis of a phase II study of venetoclax. Patients underwent PET-CT at screening and were not enrolled/treated if Richter's transformation was confirmed pathologically. Of 167 patients screened, 57 met criteria for biopsy after PET-CT. Of 35 patients who underwent biopsy, eight had Richter's transformation, two had another malignancy, and 25 had CLL. A PET-CT maximum standardized uptake value (SUVmax) ≥10 had 71% sensitivity and 50% specificity for detecting Richter's transformation [Odds Ratio (OR): 2.5, 95%CI: 0.4-15; P=0.318]. Response rate to venetoclax was similar for screening SUVmax <10 versus ≥10 (65% vs. 62%) (n=127 enrolled), though median progression-free survival was longer at <10 months (24.7 vs. 15.4 months; P=0.0335). Six patients developed Richter's transformation on venetoclax, of whom two had screening biopsy demonstrating CLL (others did not have a biopsy) and five had screening SUVmax <10. We have defined the test characteristics for PET-CT to distinguish progression of CLL as compared to Richter's transformation when biopsied in patients treated with B-cell receptor signaling pathway inhibitors. Overall diminished sensitivity and specificity as compared to prior reports of patients treated with chemotherapy/chemoimmunotherapy suggest it has diminished ability to discriminate these two diagnoses using a SUVmax ≥10 cutoff. This cutoff did not identify venetoclax-treated patients with an inferior response but may be predictive of inferior progression-free survival. (Registered at clinicaltrials.gov identifier: 02141282).
Copyright© 2019 Ferrata Storti Foundation.
Figures
References
-
- Rossi D, Cerri M, Capello D, et al. Biological and clinical risk factors of chronic lymphocytic leukaemia transformation to Richter syndrome. Br J Haematol. 2008;142(2):202–215. - PubMed
-
- Molica S. A systematic review on Richter syndrome: what is the published evidence¿ Leuk Lymphoma. 2010;51(3):415–421. - PubMed
-
- Tsimberidou AM, Kantarjian HM, Cortes J, et al. Fractionated cyclophosphamide, vincristine, liposomal daunorubicin, and dexamethasone plus rituximab and granulocyte-macrophage-colony stimulating factor (GM-CSF) alternating with methotrexate and cytarabine plus rituximab and GM-CSF in patients with Richter syndrome or fludarabine-refractory chronic lymphocytic leukemia. Cancer. 2003;97(7):1711–1720. - PubMed
-
- Tsimberidou AM, O’Brien SM, Cortes JE, et al. Phase II study of fludarabine, cytarabine (Ara-C), cyclophosphamide, cisplatin and GM-CSF (FACPGM) in patients with Richter’s syndrome or refractory lymphoproliferative disorders. Leuk Lymphoma. 2002;43(4):767–772. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
