

Rationale and protocol for estimating the economic value of a multicomponent quality improvement strategy for diabetes care in South Asia
- PMID: 30923749
- PMCID: PMC6421672
- DOI: 10.1186/s41256-019-0099-x
Rationale and protocol for estimating the economic value of a multicomponent quality improvement strategy for diabetes care in South Asia
Abstract
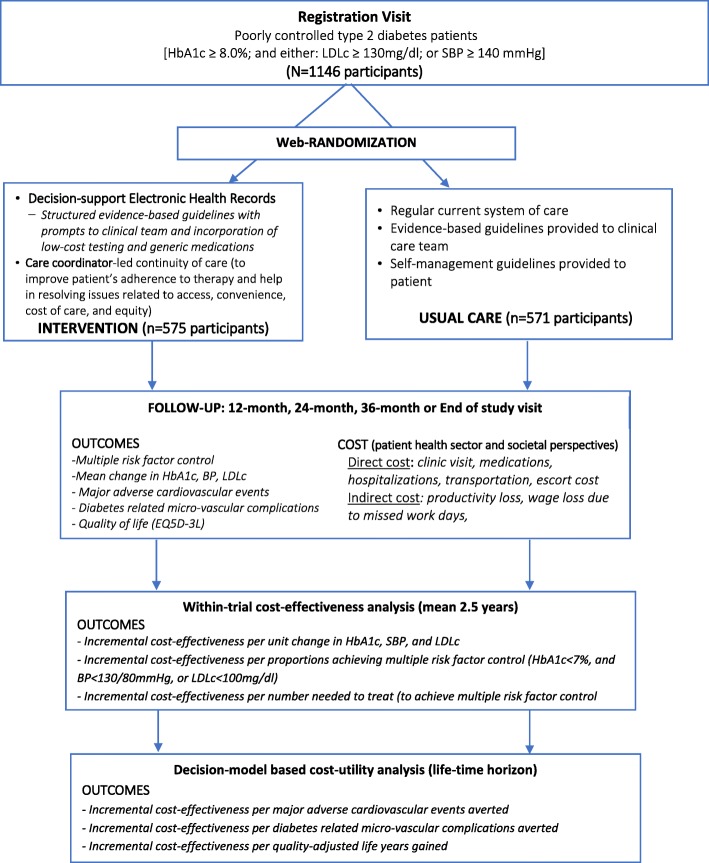
Background: Economic dimensions of implementing quality improvement for diabetes care are understudied worldwide. We describe the economic evaluation protocol within a randomised controlled trial that tested a multi-component quality improvement (QI) strategy for individuals with poorly-controlled type 2 diabetes in South Asia.
Methods/design: This economic evaluation of the Centre for Cardiometabolic Risk Reduction in South Asia (CARRS) randomised trial involved 1146 people with poorly-controlled type 2 diabetes receiving care at 10 diverse diabetes clinics across India and Pakistan. The economic evaluation comprises both a within-trial cost-effectiveness analysis (mean 2.5 years follow up) and a microsimulation model-based cost-utility analysis (life-time horizon). Effectiveness measures include multiple risk factor control (achieving HbA1c < 7% and blood pressure < 130/80 mmHg and/or LDL-cholesterol< 100 mg/dl), and patient reported outcomes including quality adjusted life years (QALYs) measured by EQ-5D-3 L, hospitalizations, and diabetes related complications at the trial end. Cost measures include direct medical and non-medical costs relevant to outpatient care (consultation fee, medicines, laboratory tests, supplies, food, and escort/accompanying person costs, transport) and inpatient care (hospitalization, transport, and accompanying person costs) of the intervention compared to usual diabetes care. Patient, healthcare system, and societal perspectives will be applied for costing. Both cost and health effects will be discounted at 3% per year for within trial cost-effectiveness analysis over 2.5 years and decision modelling analysis over a lifetime horizon. Outcomes will be reported as the incremental cost-effectiveness ratios (ICER) to achieve multiple risk factor control, avoid diabetes-related complications, or QALYs gained against varying levels of willingness to pay threshold values. Sensitivity analyses will be performed to assess uncertainties around ICER estimates by varying costs (95% CIs) across public vs. private settings and using conservative estimates of effect size (95% CIs) for multiple risk factor control. Costs will be reported in US$ 2018.
Discussion: We hypothesize that the additional upfront costs of delivering the intervention will be counterbalanced by improvements in clinical outcomes and patient-reported outcomes, thereby rendering this multi-component QI intervention cost-effective in resource constrained South Asian settings.
Trial registration: ClinicalTrials.gov: NCT01212328.
Keywords: Diabetes care; Economic evaluation; Multicomponent strategy; Quality improvement; South Asia.
Conflict of interest statement
Institutional ethics committees at each participating site and the research coordinating centres (Public Health Foundation of India and Emory University, USA) approved the study and all physicians and patients gave written informed consent prior to participating in this study.Not applicable.The authors declare that they have no competing interests.
Figures
References
-
- Deepa M, Anjana RM, Manjula D, Narayan KM, Mohan V. Convergence of prevalence rates of diabetes and cardiometabolic risk factors in middle and low income groups in urban India: 10-year follow-up of the Chennai urban population study. J Diabetes Sci Technol. 2011;5(4):918–927. doi: 10.1177/193229681100500415. - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
