

Re-emerging role of macroscopic appearance in treatment strategy for gastric cancer
- PMID: 30923781
- PMCID: PMC6422795
- DOI: 10.1002/ags3.12218
Re-emerging role of macroscopic appearance in treatment strategy for gastric cancer
Abstract
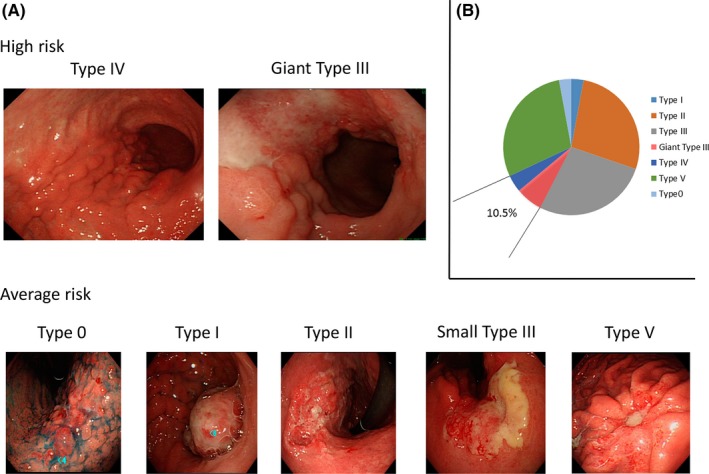
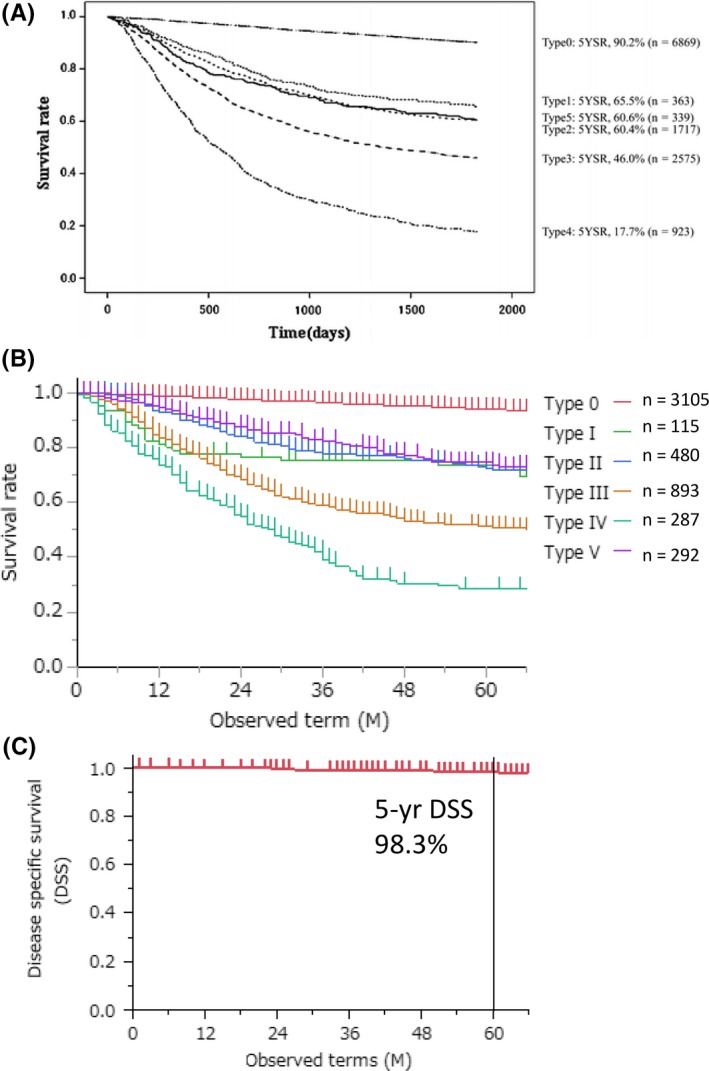
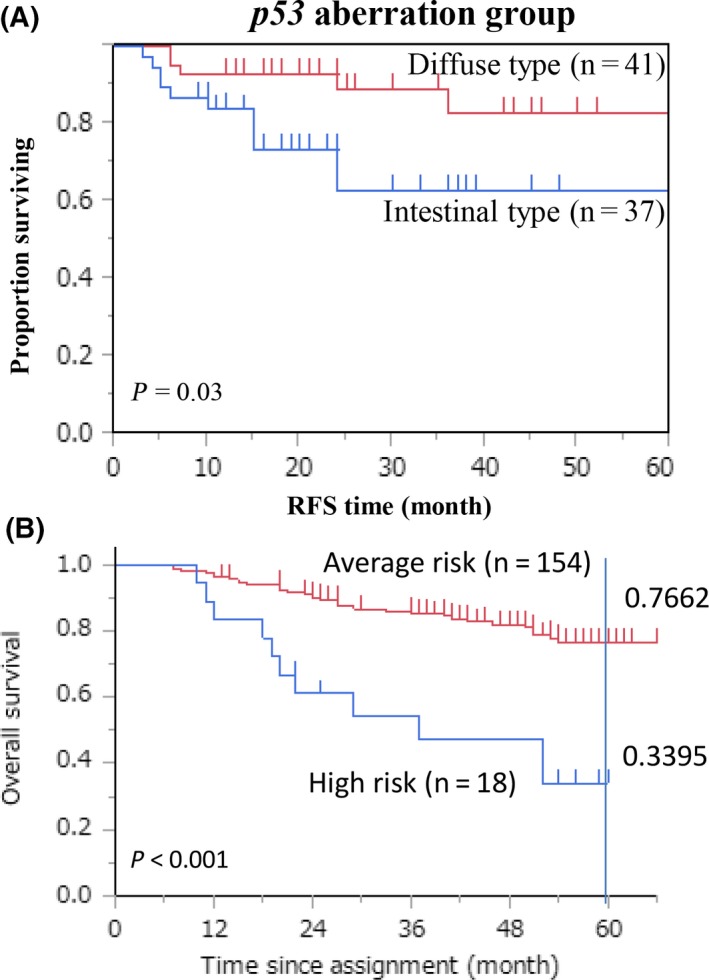
Pathological outcomes are definitely the most important prognostic factors in gastric cancer, but they can be obtained only after surgical resection. Use of preoperative adjuvant chemotherapy is becoming widespread for aggressive human cancer, so clinical factors such as macroscopic features are important as they are highly predictive for patient prognosis. In gastric cancer, the macroscopic type represents a distinct prognosis; Type 0 represents early gastric cancer with excellent prognosis, but, among advanced tumors, giant Type III and Type IV tumors have a dismal prognosis. Japan Clinical Oncology Group (JCOG) Stomach Cancer Study Group adopted macroscopic features as high-risk entities in clinical trials. It makes sense for risk classification to use macroscopic phenotypes because The Cancer Genome Atlas (TCGA) Network has lately subcategorized different histologies associated with specific macroscopic types by the molecular features of the whole genome. Dismal prognosis of Type IV gastric cancer is notorious, but similar prognosis was seen in giant Type III gastric cancer defined as 8 cm or beyond, both of which are unique for their propensity of peritoneal dissemination. In this review, clinical relevance including prognosis of such macroscopic high-risk features will be separately debated in the context of precision medicine and updated prognostic outcomes will be presented under the present standard therapy of curative surgery followed by postoperative S-1 chemotherapy. Moreover, promising emerging novel therapeutic strategies including trimodal potent regimens or intraperitoneal chemotherapy will be described for such aggressive gastric cancer.
Keywords: gastric cancer; macroscopic appearance; precision medicine; therapeutic strategy.
Conflict of interest statement
Authors declare no conflicts of interest for this article.
Figures
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. - PubMed
-
- Japanese Gastric Cancer Association . Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14(2):101–12. - PubMed
-
- Maruyama K. The most important prognostic factors for gastric cancer patients: a study using univariate and multivariate analyses. Scand J Gastroenterol. 1987;22(Supp133):63–8.
-
- Moriguchi S, Maehara Y, Korenaga D, Sugimachi K, Hayashi Y, Nose Y. Prediction of survival time after curative surgery for advanced gastric cancer. Eur J Surg Oncol. 1992;18(3):287–92. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
