

Effect on inclined medial proximal tibial articulation for varus alignment in advanced knee osteoarthritis
- PMID: 30923977
- PMCID: PMC6439040
- DOI: 10.1186/s40634-019-0180-x
Effect on inclined medial proximal tibial articulation for varus alignment in advanced knee osteoarthritis
Abstract
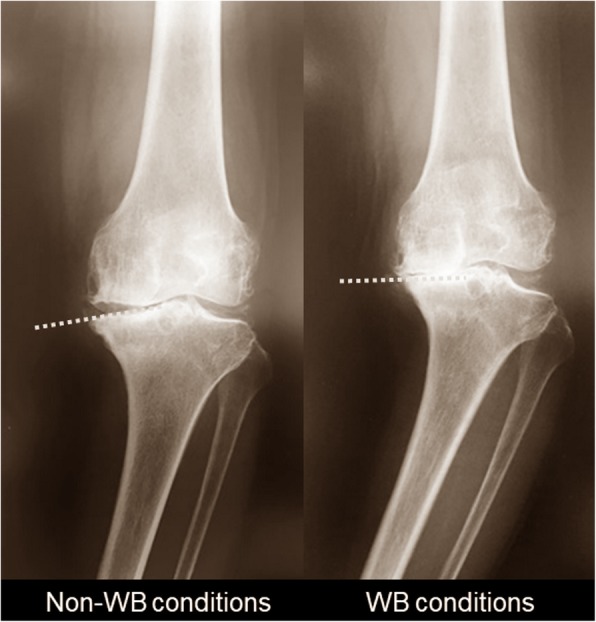
Background: The inclination of the medial compartment of the proximal tibia (MCT) is assumed to be a critical factor for varus alignment in advanced knee osteoarthritis (OA). This study was aimed at investigating; (1) whether the inclination of MCT is aligned parallel to the ground under weight-bearing (WB) conditions; (2) whether this is associated with the change in alignment and the relative position between the bones; and (3) whether the tibia or femur mainly contributes to the changes.
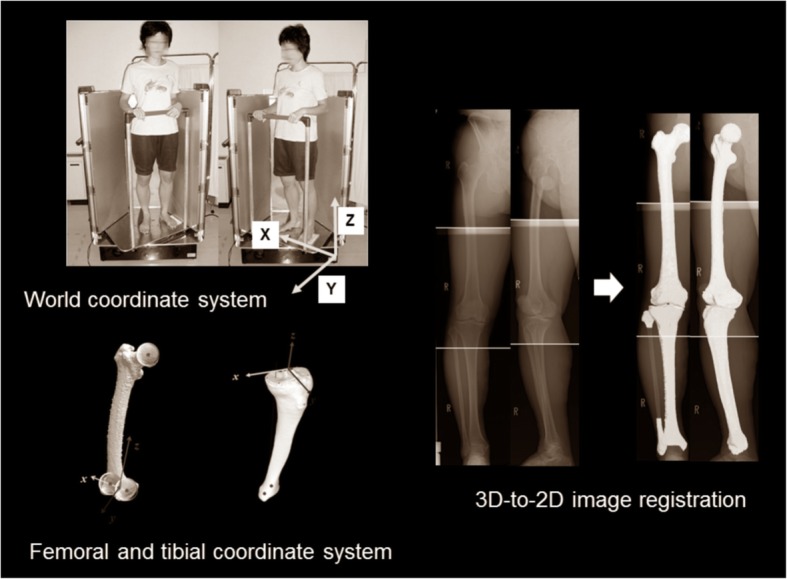
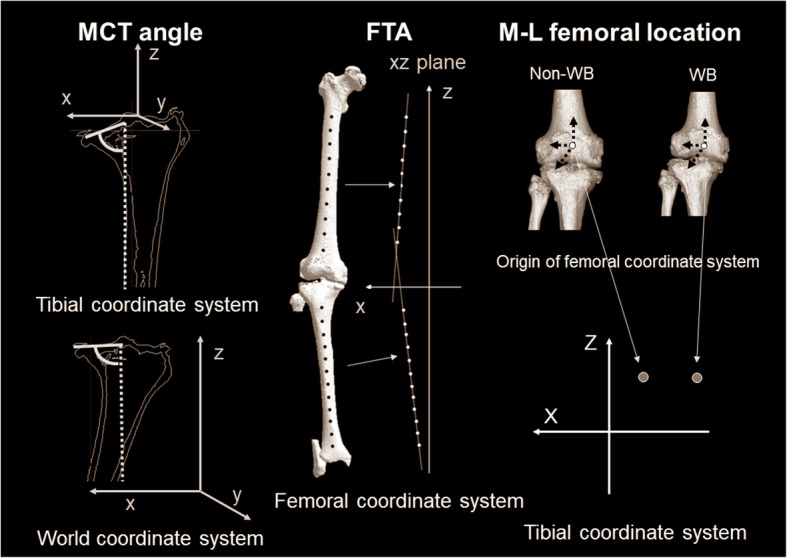
Methods: We examined 102 knees (84 women, 18 men; mean 75 years). A three-dimensional (3D) assessment system was applied on biplanar whole lower extremity radiographies using 3D-to-2D image registration technique. The evaluation parameters were 1) MCT angle, 2) femorotibial angle (FTA), 3) medial-lateral femoral location to the tibia (M-L femoral location), 4) WB line passing point, and 5) tibial position to WB line (tibial position) and 6) femoral postion to WB line (femoral position). Each parameter was evaluated in non-WB and WB conditions, and the differences (Δ-parameters).
Results: MCT angle in the world coordinate system was larger than that in the tibial coordinate system (p < 0.0001). ΔMCT angle was correlated with ΔFTA (p = 0.002) and ΔM-L femoral location (p = 0.004). The tibial position was the more dominant factor for ΔMCT angle (p = 0.001), ΔFTA (p < 0.0001), and ΔWB line passing point (p < 0.0001) .
Conclusions: The inclination in MCT was aligned parallel to the ground under WB conditions (tibial parallel phenomenon). The parallel phenomenon was associated with the change of alignment and the relative position between the bones in the coronal plane. These phenomena were produced mainly by the tibia, not the femur.
Level of evidence: Level IV.
Keywords: Inclination in the medial compartment of the proximal tibia; Knee osteoarthritis; Tibial parallel phenomenon; Varus alignment; Weight-bearing conditions.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Institutional Review Board in Niigata University. Appropriate consents, permissions and releases were obtained.
Consent for publication
All presentations had consent to publish.
Competing interests
The authors did not receive and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials
