

Tobacco Smoking and Mortality in Asia: A Pooled Meta-analysis
- PMID: 30924901
- PMCID: PMC6450311
- DOI: 10.1001/jamanetworkopen.2019.1474
Tobacco Smoking and Mortality in Asia: A Pooled Meta-analysis
Abstract
Importance: Understanding birth cohort-specific tobacco smoking patterns and their association with total and cause-specific mortality is important for projecting future deaths due to tobacco smoking across Asian populations.
Objectives: To assess secular trends of tobacco smoking by countries or regions and birth cohorts and evaluate the consequent mortality in Asian populations.
Design, setting, and participants: This pooled meta-analysis was based on individual participant data from 20 prospective cohort studies participating in the Asia Cohort Consortium. Between September 1, 2017, and March 31, 2018, a total of 1 002 258 Asian individuals 35 years or older were analyzed using Cox proportional hazards regression analysis and random-effects meta-analysis. The pooled results were presented for mainland China; Japan; Korea, Singapore, and Taiwan; and India.
Exposures: Tobacco use status, age at starting smoking, number of cigarettes smoked per day, and age at quitting smoking.
Main outcomes and measures: Country or region and birth cohort-specific mortality and the population attributable risk for deaths from all causes and from lung cancer.
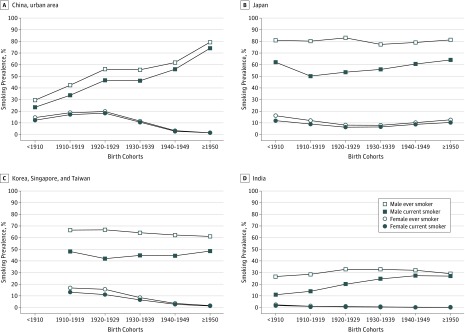
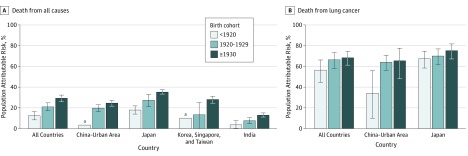
Results: Of 1 002 258 participants (51.1% women and 48.9% men; mean [SD] age at baseline, 54.6 [10.4] years), 144 366 deaths (9158 deaths from lung cancer) were ascertained during a mean (SD) follow-up of 11.7 (5.3) years. Smoking prevalence for men steadily increased in China and India, whereas it plateaued in Japan and Korea, Singapore, and Taiwan. Among Asian male smokers, the mean age at starting smoking decreased in successive birth cohorts, while the mean number of cigarettes smoked per day increased. These changes were associated with an increasing relative risk of death in association with current smoking in successive birth cohorts of pre-1920, 1920s, and 1930 or later, with hazard ratios for all-cause mortality of 1.26 (95% CI, 1.17-1.37) for the pre-1920 birth cohort, 1.47 (95% CI, 1.35-1.61) for the 1920s birth cohort, and 1.70 (95% CI, 1.57-1.84) for the cohort born in 1930 or later. The hazard ratios for lung cancer mortality were 3.38 (95% CI, 2.25-5.07) for the pre-1920 birth cohort, 4.74 (95% CI, 3.56-6.32) for the 1920s birth cohort, and 4.80 (95% CI, 3.71-6.19) for the cohort born in 1930 or later. Tobacco smoking accounted for 12.5% (95% CI, 8.4%-16.3%) of all-cause mortality in the pre-1920 birth cohort, 21.1% (95% CI, 17.3%-24.9%) of all-cause mortality in the 1920s birth cohort, and 29.3% (95% CI, 26.0%-32.3%) of all-cause mortality for the cohort born in 1930 or later. Tobacco smoking among men accounted for 56.6% (95% CI, 44.7%-66.3%) of lung cancer mortality in the pre-1920 birth cohort, 66.6% (95% CI, 58.3%-73.5%) of lung cancer mortality in the 1920s birth cohort, and 68.4% (95% CI, 61.3%-74.4%) of lung cancer mortality for the cohort born in 1930 or later. For women, tobacco smoking patterns and lung cancer mortality varied substantially by countries and regions.
Conclusions and relevance: In this study, mortality associated with tobacco smoking continued to increase among Asian men in recent birth cohorts, indicating that tobacco smoking will remain a major public health problem in most Asian countries in the coming decades. Implementing comprehensive tobacco-control programs is warranted to end the tobacco epidemic.
Conflict of interest statement
Figures
Comment in
-
Tobacco Smoking in Asia-A Public Health Threat.JAMA Netw Open. 2019 Mar 1;2(3):e191471. doi: 10.1001/jamanetworkopen.2019.1471. JAMA Netw Open. 2019. PMID: 30924888 No abstract available.
References
-
- World Health Organization WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco Use and Prevention Policies Geneva, Switzerland: World Health Organization; 2017.
-
- Eriksen M, Mackay J, Schluger NW. The Tobacco Atlas. 5th ed Atlanta, GA: American Cancer Society; 2015.
-
- World Health Organization WHO Framework Convention on Tobacco Control. Geneva, Switzerland: World Health Organization; 2005.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
