

Lipid Accumulation and Chronic Kidney Disease
- PMID: 30925738
- PMCID: PMC6520701
- DOI: 10.3390/nu11040722
Lipid Accumulation and Chronic Kidney Disease
Abstract
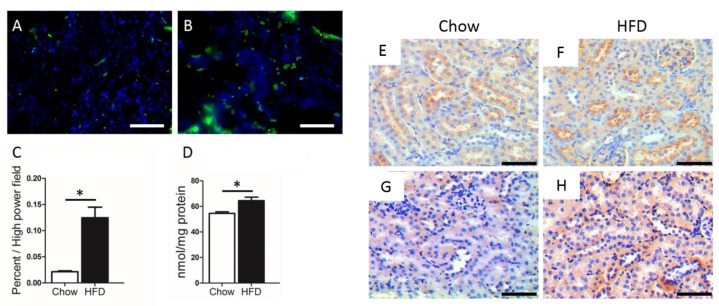
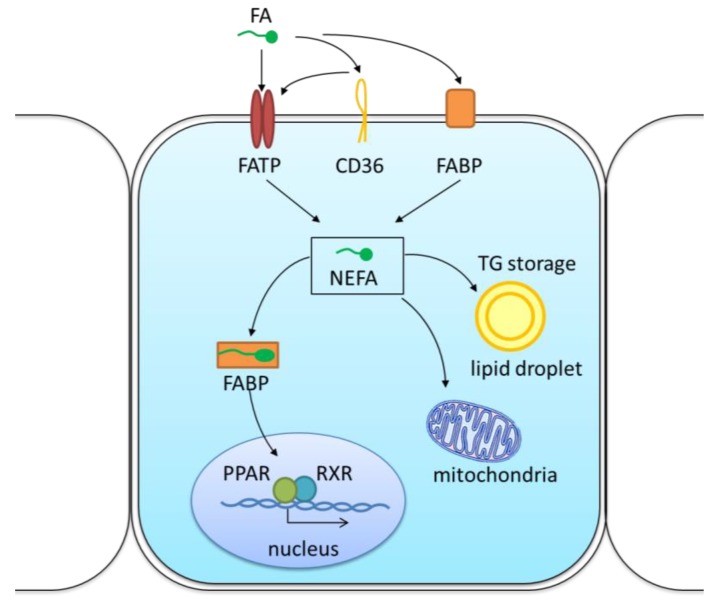
Obesity and hyperlipidemia are the most prevalent independent risk factors of chronic kidney disease (CKD), suggesting that lipid accumulation in the renal parenchyma is detrimental to renal function. Non-esterified fatty acids (also known as free fatty acids, FFA) are especially harmful to the kidneys. A concerted, increased FFA uptake due to high fat diets, overexpression of fatty acid uptake systems such as the CD36 scavenger receptor and the fatty acid transport proteins, and a reduced β-oxidation rate underlie the intracellular lipid accumulation in non-adipose tissues. FFAs in excess can damage podocytes, proximal tubular epithelial cells and the tubulointerstitial tissue through various mechanisms, in particular by boosting the production of reactive oxygen species (ROS) and lipid peroxidation, promoting mitochondrial damage and tissue inflammation, which result in glomerular and tubular lesions. Not all lipids are bad for the kidneys: polyunsaturated fatty acids (PUFA) such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) seem to help lag the progression of chronic kidney disease (CKD). Lifestyle interventions, especially dietary adjustments, and lipid-lowering drugs can contribute to improve the clinical outcome of patients with CKD.
Keywords: blood lipids; chronic kidney disease; lipid accumulation; metabolic disease; potential therapeutic strategy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- National Kidney Foundation K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002;39(Suppl. 1):S1–S266. - PubMed
-
- Collins A.J., Foley R.N., Chavers B., Gilbertson D., Herzog C., Johansen K., Kasiske B., Kutner N., Liu J., St Peter W., et al. United States Renal Data System 2011 Annual Data Report: Atlas of chronic kidney disease & end-stage renal disease in the United States. Am. J. Kidney Dis. 2012;59(Suppl. 1):e1–e420. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
