

"Practice so that the skill does not disappear": mixed methods evaluation of simulator-based learning for midwives in Uganda
- PMID: 30925890
- PMCID: PMC6440002
- DOI: 10.1186/s12960-019-0350-z
"Practice so that the skill does not disappear": mixed methods evaluation of simulator-based learning for midwives in Uganda
Abstract
Background: Postpartum hemorrhage and neonatal asphyxia are leading causes of maternal and neonatal mortality, respectively, that occur relatively rarely in low-volume health facilities in sub-Saharan Africa. Rare occurrence of cases may limit the readiness and skills that individual birth attendants have to address complications. Evidence suggests that simulator-based training and practice sessions can help birth attendants maintain these life-saving skills; one approach is called "low-dose, high-frequency" (LDHF). The objective of this evaluation is to determine the facilitating factors and barriers to participation in LDHF practice, using qualitative and quantitative information.
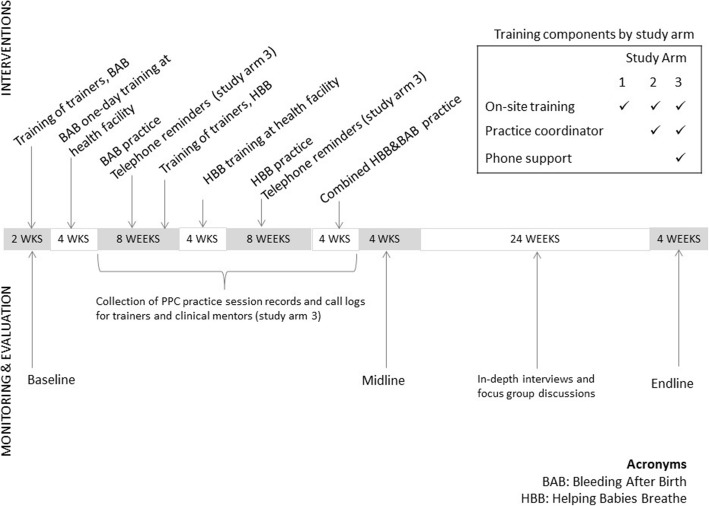
Methods: A trial in 125 facilities in Uganda compared three strategies of support for LDHF practice to improve retention of skills in prevention and treatment of postpartum hemorrhage and neonatal asphyxia. Birth attendants kept written logs of their simulator-based practice sessions, which were entered into a database, then analyzed using Stata to compare frequency of practice by the study arm. The evaluation also included 29 in-depth interviews and 19 focus group discussions with birth attendants and district trainers. Transcripts were entered in Atlas.ti software for coding, then analyzed using content analysis to identify factors that motivated or discouraged simulator-based practice.
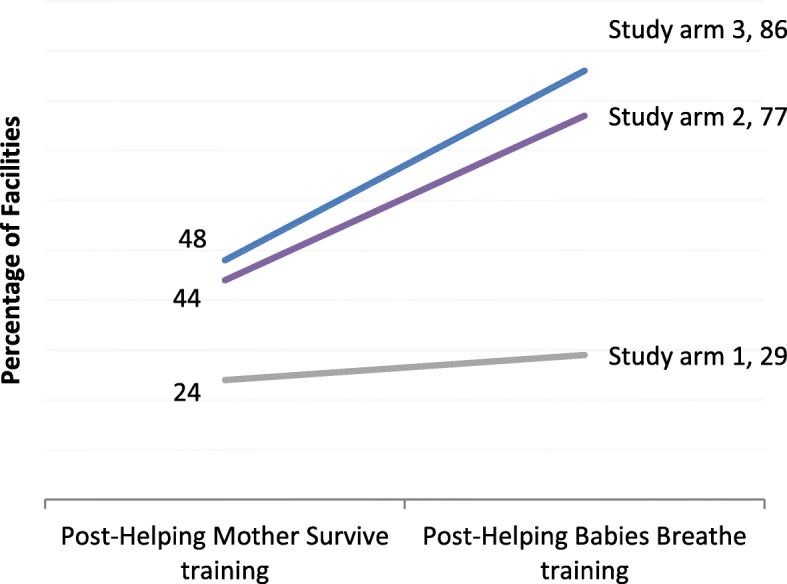
Results: Practice log data indicated that simulator-based practice sessions occurred more frequently in facilities where one or two practice coordinators helped schedule and lead the practice sessions and in health centers compared to hospitals. The qualitative data suggest that birth attendants who practiced more were motivated by a desire to maintain skills and be prepared for emergencies, external recognition, and establishing a set schedule. Barriers to consistent practice included low staffing levels, heavy workloads, and a sense that competency can be maintained through routine clinical care alone. Some facilities described norms around continuing education and some did not.
Conclusions: Designating practice coordinators to lead their peers in simulator-based practice led to more consistent skills practice within frontline health facilities. Ongoing support, scheduling of practice sessions, and assessment and communication of motivation factors may help sustain LDHF practice and similar forms of continuing professional development.
Trial registration: Registered with clinicaltrials.gov #NCT03254628 on August 18, 2018 (registered retrospectively).
Conflict of interest statement
Ethics approval and consent to participate
Institutional Reviews Boards at the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland, United States, and Makerere University in Kampala, Uganda and the Ugandan government approved this study. All participants provided verbal informed consent prior to participation, as per the approved protocol. The study is registered on
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Ubos UB of S-, ICF . Uganda Demographic and Health Survey 2016. 2018.
-
- World Health Organization . Standards for improving quality of maternal and newborn care in health facilities. Geneva: World Health Organization; 2016.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
