

Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials
- PMID: 30926892
- PMCID: PMC6441028
- DOI: 10.1038/s41598-019-41854-2
Efficacy and Safety of Pioglitazone Monotherapy in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials
Abstract
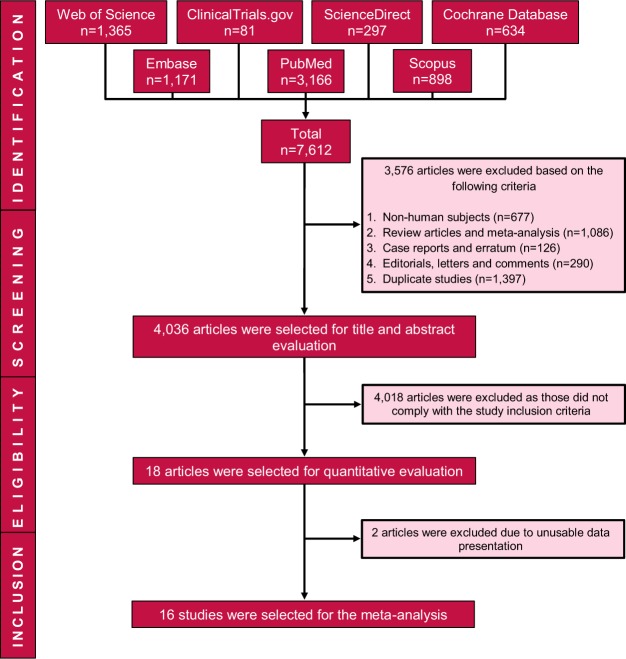
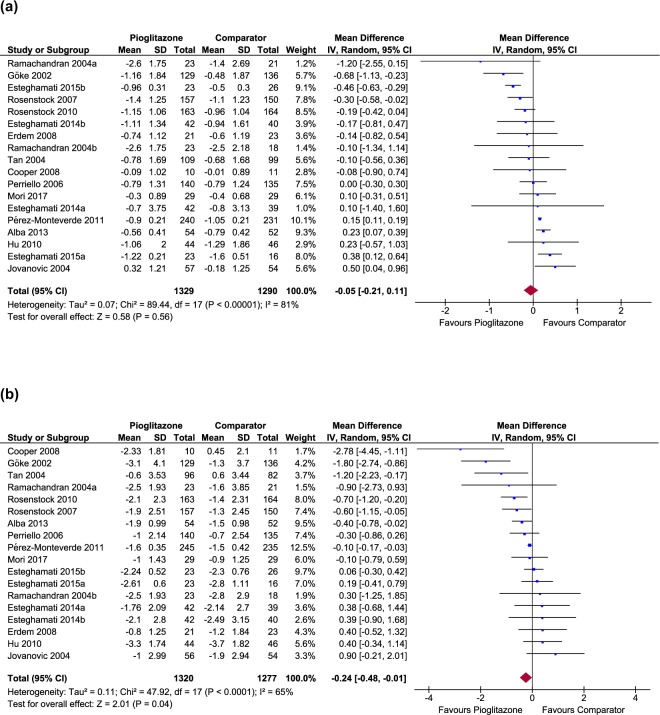
Pioglitazone, the only thiazolidinedione drug in clinical practice is under scrutiny due to reported adverse effects, it's unique insulin sensitising action provides rationale to remain as a therapeutic option for managing type 2 diabetes mellitus (T2DM). We conducted a systematic review and meta-analysis comparing pioglitazone monotherapy with monotherapies of other oral antidiabetic drugs for assessing its efficacy and safety in T2DM patients. Mean changes in glycated haemoglobin (HbA1c), and mean changes in fasting blood sugar (FBS) level, body weight (BW) and homeostasis model assessment-insulin resistance (HOMA-IR) were primary and secondary outcomes, respectively. Safety outcomes were changes in lipid parameters, blood pressure and incidences of adverse events. Metafor package of R software and RevMan software based on random-effects model were used for analyses. We included 16 randomised controlled trials. Pioglitazone monotherapy showed equivalent efficacy as comparators in reducing HbA1c by 0.05% (95% CI: -0.21 to 0.11) and greater efficacy in reducing FBS level by 0.24 mmol/l (95% CI: -0.48 to -0.01). Pioglitazone showed similar efficacy as comparators in reducing HOMA-IR (WMD: 0.05, 95% CI: -0.49 to 0.59) and increasing high-density lipoprotein level (WMD: 0.02 mmol/l, 95% CI: -0.06 to 0.10). Improved blood pressure (WMD: -1.05 mmHg, 95% CI: -4.29 to 2.19) and triglycerides level (WMD: -0.71 mmol/l, 95% CI: -1.70 to 0.28) were also observed with pioglitazone monotherapy. There was a significant association of pioglitazone with increased BW (WMD: 2.06 kg, 95% CI: 1.11 to 3.01) and risk of oedema (RR: 2.21, 95% CI: 1.48 to 3.31), though the risk of hypoglycaemia was absolutely lower (RR: 0.51, 95% CI: 0.33 to 0.80). Meta-analysis supported pioglitazone as an effective treatment option for T2DM patients to ameliorate hyperglycaemia, adverse lipid metabolism and blood pressure. Pioglitazone is suggested to prescribe following individual patient's needs. It can be a choice of drug for insulin resistant T2DM patients having dyslipidaemia, hypertension or history of cardiovascular disease.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
