

Sex-based differences in outcomes, 30-day readmissions, and costs following catheter ablation of atrial fibrillation: the United States Nationwide Readmissions Database 2010-14
- PMID: 30927423
- PMCID: PMC7963138
- DOI: 10.1093/eurheartj/ehz151
Sex-based differences in outcomes, 30-day readmissions, and costs following catheter ablation of atrial fibrillation: the United States Nationwide Readmissions Database 2010-14
Abstract
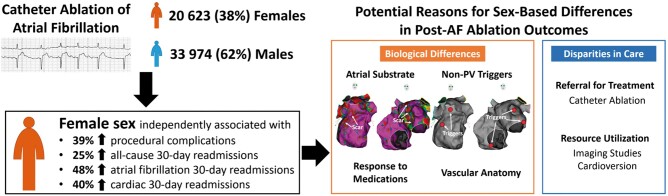
Aims: Although catheter ablation has emerged as an important therapy for patients with symptomatic atrial fibrillation (AF), there are limited data on sex-based differences in outcomes. We sought to compare in-hospital outcomes and 30-day readmissions of women and men undergoing AF ablation.
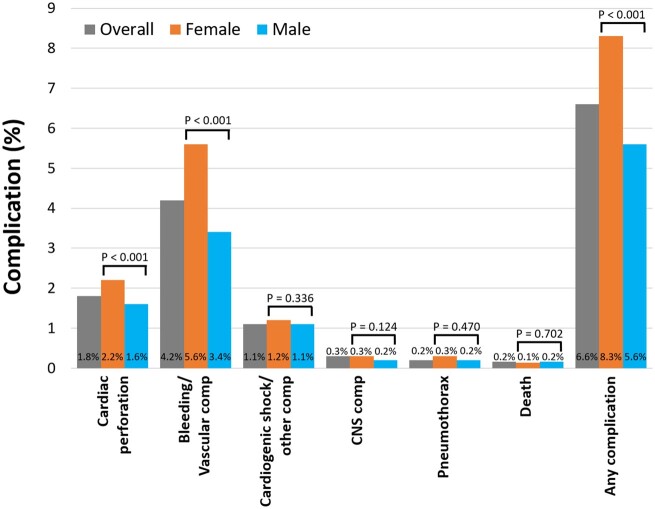
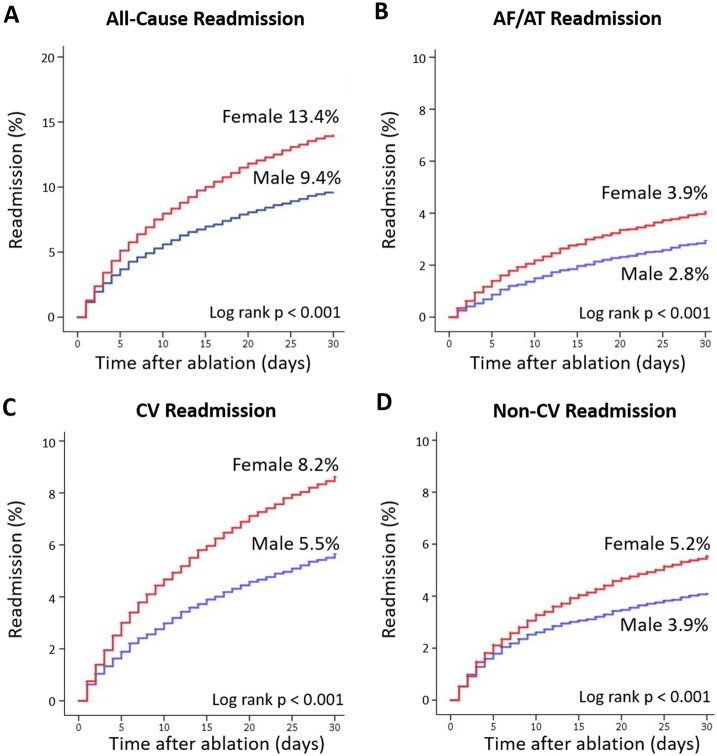
Methods and results: Using the United States Nationwide Readmissions Database, we analysed patients undergoing AF ablation between 2010 and 2014. Based on ICD-9-CM codes, we identified co-morbidities and outcomes. Multivariable logistic regression and inverse probability-weighting analysis were performed to assess female sex as a predictor of endpoints. Of 54 597 study patients, 20 623 (37.7%) were female. After adjustment for age, co-morbidities, and hospital factors, women had higher rates of any complication [adjusted odds ratio (aOR) 1.39; P < 0.0001], cardiac perforation (aOR 1.39; P = 0.006), and bleeding/vascular complications (aOR 1.49; P < 0.0001). Thirty-day all-cause readmission rates were higher for women compared to men (13.4% vs. 9.4%; P < 0.0001). Female sex was independently associated with readmission for AF/atrial tachycardia (aOR 1.48; P < 0.0001), cardiac causes (aOR 1.40; P < 0.0001), and all causes (aOR 1.25; P < 0.0001). Similar findings were confirmed with inverse probability-weighting analysis. Despite increased complications and readmissions, total costs for AF ablation were lower for women than men due to decreased resource utilization.
Conclusions: Independent of age, co-morbidities, and hospital factors, women have higher rates of complications and readmissions following AF ablation. Sex-based differences and disparities in the management of AF need to be explored to address these gaps in outcomes.
Keywords: Atrial fibrillation; Mortality; Outcomes research; Readmission; Sex.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2019. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Peri-procedural complications in women: an alarming and consistent trend.Eur Heart J. 2019 Sep 21;40(36):3044-3045. doi: 10.1093/eurheartj/ehz193. Eur Heart J. 2019. PMID: 31004157 Free PMC article. No abstract available.
References
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton-Cheh C, Lubitz SA, Magnani JW, Ellinor PT, Seshadri S, Wolf PA, Vasan RS, Benjamin EJ, Levy D. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet 2015;386:154–162. - PMC - PubMed
-
- Piccini JP, Simon DN, Steinberg BA, Thomas L, Allen LA, Fonarow GC, Gersh B, Hylek E, Kowey PR, Reiffel JA, Naccarelli GV, Chan PS, Spertus JA, Peterson ED. Outcomes registry for better informed treatment of atrial fibrillation I and patients. Differences in clinical and functional outcomes of atrial fibrillation in women and men: two-year results from the ORBIT-AF registry. JAMA Cardiol 2016;1:282–291. - PubMed
-
- Humphries KH, Kerr CR, Connolly SJ, Klein G, Boone JA, Green M, Sheldon R, Talajic M, Dorian P, Newman D. New-onset atrial fibrillation: sex differences in presentation, treatment, and outcome. Circulation 2001;103:2365–2370. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener H-C, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GYH, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:2893–2962. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
