

Evidence that antibiotic administration is effective in the treatment of a subset of patients with intra-amniotic infection/inflammation presenting with cervical insufficiency
- PMID: 30928565
- PMCID: PMC7218799
- DOI: 10.1016/j.ajog.2019.03.017
Evidence that antibiotic administration is effective in the treatment of a subset of patients with intra-amniotic infection/inflammation presenting with cervical insufficiency
Abstract
Background: Cervical insufficiency is a risk factor for spontaneous midtrimester abortion or early preterm birth. Intra-amniotic infection has been reported in 8-52% of such patients and intra-amniotic inflammation in 81%. Some professional organizations have recommended perioperative antibiotic treatment when emergency cervical cerclage is performed. The use of prophylactic antibiotics is predicated largely on the basis that they reduce the rate of complications during the course of vaginal surgery. However, it is possible that antibiotic administration can also eradicate intra-amniotic infection/inflammation and improve pregnancy outcome.
Objective: To describe the outcome of antibiotic treatment in patients with cervical insufficiency and intra-amniotic infection/inflammation.
Study design: The study population consisted of 22 women who met the following criteria: (1) singleton pregnancy; (2) painless cervical dilatation of >1 cm between 16.0 and 27.9 weeks of gestation; (3) intact membranes and absence of uterine contractions; (4) transabdominal amniocentesis performed for the evaluation of the microbiologic and inflammatory status of the amniotic cavity; (5) presence of intra-amniotic infection/inflammation; and (6) antibiotic treatment (regimen consisted of ceftriaxone, clarithromycin, and metronidazole). Amniotic fluid was cultured for aerobic and anaerobic bacteria and genital mycoplasmas, and polymerase chain reaction for Ureaplasma spp. was performed. Intra-amniotic infection was defined as a positive amniotic fluid culture for microorganisms or a positive polymerase chain reaction for Ureaplasma spp., and intra-amniotic inflammation was suspected when there was an elevated amniotic fluid white blood cell count (≥19 cells/mm3) or a positive rapid test for metalloproteinase-8 (sensitivity 10 ng/mL). For the purpose of this study, the "gold standard" for diagnosis of intra-amniotic inflammation was an elevated interleukin-6 concentration (>2.6 ng/mL) using an enzyme-linked immunosorbent assay. The results of amniotic fluid interleukin-6 were not available to managing clinicians. Follow-up amniocentesis was routinely offered to monitor the microbiologic and inflammatory status of the amniotic cavity and fetal lung maturity. Treatment success was defined as resolution of intra-amniotic infection/inflammation or delivery ≥34 weeks of gestation.
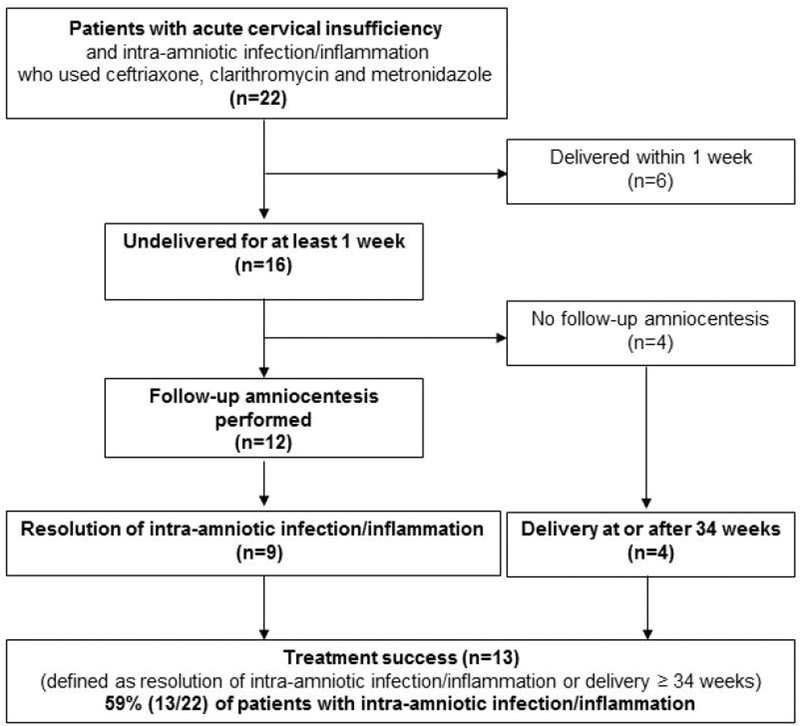
Results: Of 22 patients with cervical insufficiency and intra-amniotic infection/inflammation, 3 (14%) had microorganisms in the amniotic fluid. Of the 22 patients, 6 (27%) delivered within 1 week of amniocentesis and the remaining 16 (73%) delivered more than 1 week after the diagnostic procedure. Among these, 12 had a repeat amniocentesis to assess the microbial and inflammatory status of the amniotic cavity; in 75% (9/12), there was objective evidence of resolution of intra-amniotic inflammation or intra-amniotic infection demonstrated by analysis of amniotic fluid at the time of the repeat amniocentesis. Of the 4 patients who did not have a follow-up amniocentesis, all delivered ≥34 weeks, 2 of them at term; thus, treatment success occurred in 59% (13/22) of cases.
Conclusion: In patients with cervical insufficiency and intra-amniotic infection/inflammation, administration of antibiotics (ceftriaxone, clarithromycin, and metronidazole) was followed by resolution of the intra-amniotic inflammatory process or intra-amniotic infection in 75% of patients and was associated with treatment success in about 60% of cases.
Keywords: Antimicrobial agents; MMP-8; Ureaplasma urealyticum, chorioamnionitis; amniotic fluid; biomarker; ceftriaxone; cephalosporins; cerclage; clarithromycin; interleukin-6; metronidazole; pregnancy; prematurity.
Published by Elsevier Inc.
Conflict of interest statement
Figures
Comment in
-
Successful treatment of intraamniotic infection/inflammation: a paradigm shift.Am J Obstet Gynecol. 2019 Aug;221(2):83-85. doi: 10.1016/j.ajog.2019.05.020. Am J Obstet Gynecol. 2019. PMID: 31358235 No abstract available.
References
-
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No.142: Cerclage for the management of cervical insufficiency. Obstetrics and gynecology 2014;123:372–9. - PubMed
-
- Althuisius SM, Dekker GA, Hummel P, van Geijn HP, Cervical incompetence prevention randomized cerclage t. Cervical incompetence prevention randomized cerclage trial: emergency cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol 2003;189:907–10. - PubMed
-
- Guzman ER, Houlihan C, Vintzileos A, Ivan J, Benito C, Kappy K. The significance of transvaginal ultrasonographic evaluation of the cervix in women treated with emergency cerclage. Am J Obstet Gynecol 1996;175:471–6. - PubMed
-
- Lipitz S, Libshitz A, Oelsner G, et al. Outcome of second-trimester, emergency cervical cerclage in patients with no history of cervical incompetence. Am J Perinatol 1996;13:419–22. - PubMed
-
- Latta RA, McKenna B. Emergent cervical cerclage: predictors of success or failure. J Matern Fetal Med 1996;5:22–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
