

Primary vitreoretinal lymphoma
- PMID: 30930667
- PMCID: PMC6424706
- DOI: 10.1016/j.sjopt.2018.12.008
Primary vitreoretinal lymphoma
Abstract
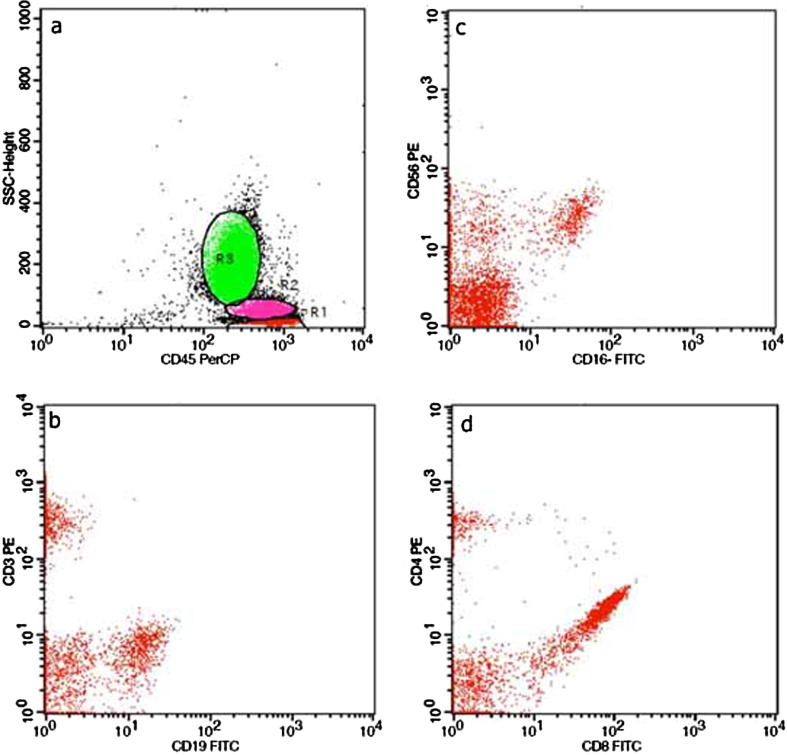
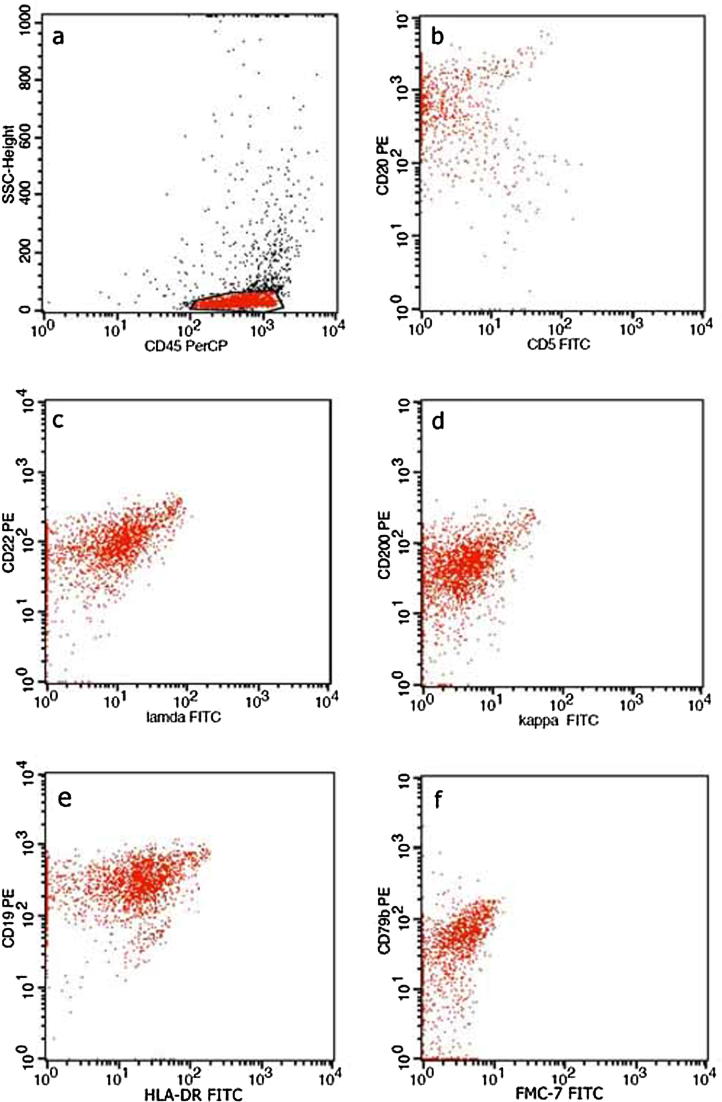
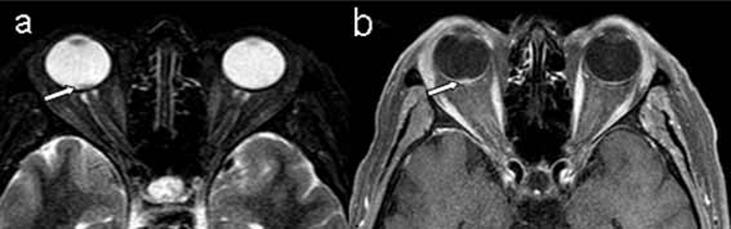
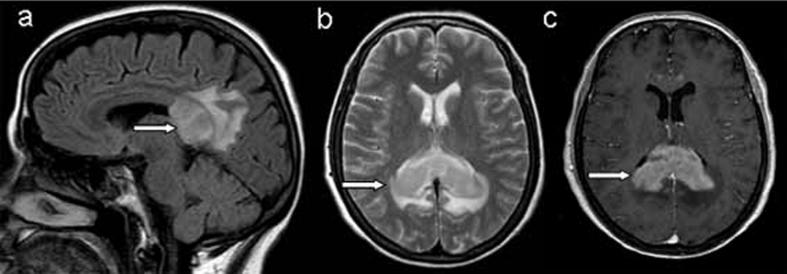
Primary vitreoretinal lymphoma (PVRL) is a rare ocular lymphoid malignancy, which consists a subset of primary central system lymphoma (PCNSL) and the most common type of intraocular lymphoma. The involvement of eyes is estimated to be approximately 20% of PCNSL, but the brain involvement may be up to 80% of PVRL. Typically, PVRL is a high grade B-cell malignancy of the retina and needs to be assorted from choroidal low-grade B-cell lymphomas. Very often PVRL masquerades and can be erroneously diagnosed as chronic uveitis, white dot syndromes or other neoplasms. Establishing an accurate diagnosis may involve cytology/pathology, immunohistochemistry, flow cytometry, molecular pathology and cytokine profile analysis. There is inadequate information about PVRL's true incidence, ethnic/geographical variation and pathogenetic mechanisms. The therapeutic approach of PVRL involves aggressive chemotherapy and radiation therapy. Although PVRL tends to have a good response to the initial treatment, the prognosis is poor and the survival restricted due to the high relapse rates and CNS involvement.
Keywords: B-cell lymphoma; Intraocular lymphoma; Masquerade syndrome; Primary CNS lymphoma; Primary vitreoretinal lymphoma.
Figures
References
-
- Coupland S.E., Damato B. Understanding intraocular lymphomas. Clin Experiment Ophthalmol. 2008;36:564–578. - PubMed
-
- Sagoo M.S., Mehta H., Swampillai A.J. Primary intraocular lymphoma. Surv Ophthalmol. 2014;59:503–516. - PubMed
-
- Aziz H.A., Peereboom D.M., Singh A.D. Primary central nervous system lymphoma. Int Ophthalmol Clin. 2015;55:111–121. - PubMed
-
- Fend F., Ferreri A.J., Coupland S.E. How we diagnose and treat vitreoretinal lymphoma. Br J Haematol. 2016;173:680–692. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
