

Immune Dysfunction and Albumin-Related Immunity in Liver Cirrhosis
- PMID: 30930689
- PMCID: PMC6410448
- DOI: 10.1155/2019/7537649
Immune Dysfunction and Albumin-Related Immunity in Liver Cirrhosis
Abstract
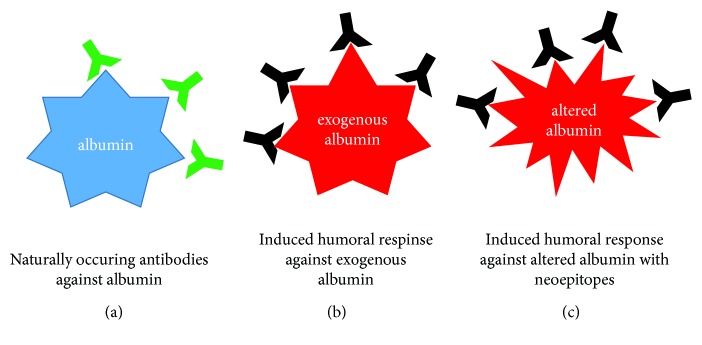
Liver cirrhosis yearly causes 1.2 million deaths worldwide, ranking as the 10th leading cause of death in the most developed countries. High susceptibility to infections along with a significant risk for infection-related mortality justifies the description of liver cirrhosis as the world's most common immunodeficiency syndrome. Liver cirrhosis is an end-stage organic disease hallmarked by a multifaceted immune dysfunction due to deterioration of antimicrobial recognition and elimination mechanisms in macrophages along with an impaired antigen presentation ability in circulating monocytes. Bacterial translocation supports-and is supported by-uncontrolled activation of immune cell responses and/or loss of toll-like receptor (TLR) tolerance, which can turn exaggerated inflammatory responses to systemic inflammation. Lipopolysaccharide (LPS) or endotoxin boosts systemic inflammatory activity through activation of TLR-2- and TLR-4-dependent pathways and facilitate a massive production of cytokines. This, in turn, results into elevated secretion of reactive oxygen species (ROS), which further enhances intestinal hyperpermeability and thus sustains a vicious circle of events widely known as "leaky gut." Albumin can be of particular benefit in cirrhotic patients with spontaneous bacterial peritonitis and/or hepatorenal syndrome type of acute kidney injury (HRS-AKI) due to anti-inflammatory and antioxidative stress as well as volume-expanding properties and endothelial-stabilizing attributes. However, presence of autoantibodies against albumin in patients with liver cirrhosis has been described. Although previous research suggested that these antibodies should be regarded as naturally occurring antibodies (NOA), the origin of the antialbumin immune response is obscure. High occurrence of NAO/albumin complexes in patients with liver disease might reflect a limited clearance capacity due to bypassing portal circulation. Moreover, high burden of oxidized albumin is associated with less favorable outcome in patients with liver cirrhosis. To date, there is no data available as to whether oxidized forms of albumin result in neoepitopes recognized by the immune system. Nevertheless, it is reasonable to hypothesize that these alterations may have the potential to induce antialbumin immune responses and thus favor systemic inflammation.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
