

Auditory Brainstem Implantation: An Overview
- PMID: 30931229
- PMCID: PMC6438789
- DOI: 10.1055/s-0039-1679891
Auditory Brainstem Implantation: An Overview
Abstract
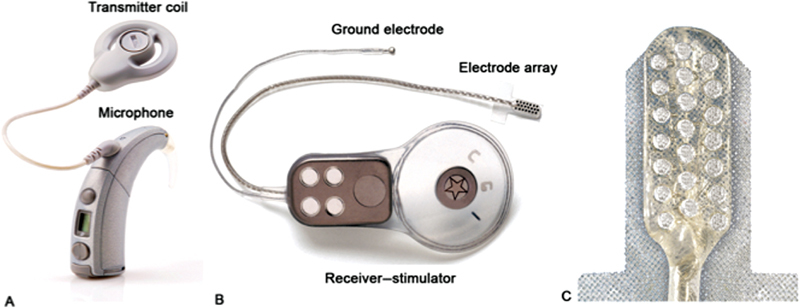
An auditory brainstem implant (ABI) is a surgically implanted central neural auditory prosthesis for the treatment of profound sensorineural hearing loss in children and adults who are not cochlear implant candidates due to a lack of anatomically intact cochlear nerves or implantable cochleae. The device consists of a multielectrode surface array which is placed within the lateral recess of the fourth ventricle along the brainstem and directly stimulates the cochlear nucleus, thereby bypassing the peripheral auditory system. In the United States, candidacy criteria for ABI include deaf patients with neurofibromatosis type 2 (NF2) who are 12 years or older undergoing first- or second-side vestibular schwannoma resection. In recent years, several non-NF2 indications for ABI have been explored, including bilateral cochlear nerve avulsion from trauma, complete ossification of the cochlea due to meningitis, or a severe cochlear malformation not amenable to cochlear implantation. In addition, growing experience with ABI in infants and children has been documented with encouraging outcomes. While cochlear implantation generally remains the first-line option for hearing rehabilitation in NF2 patients with stable tumors or post hearing preservation surgery where hearing is lost but a cochlear nerve remains accessible for stimulation, an ABI is the next alternative in cases where the cochlear nerve is absent and/or if the cochlea cannot be implanted. Herein, we review ABI device design, clinical evaluation, indications, operative technique, and outcomes as it relates to lateral skull base pathology.
Keywords: auditory brainstem implant; auditory nerve; auditory prosthesis; electric stimulation; hearing loss; neurofibromatosis type 2.
Conflict of interest statement
Figures
References
-
- Hitselberger W E, House W F, Edgerton B J, Whitaker S. Cochlear nucleus implants. Otolaryngol Head Neck Surg. 1984;92(01):52–54. - PubMed
-
- House W F, Hitselberger W E. Twenty-year report of the first auditory brain stem nucleus implant. Ann Otol Rhinol Laryngol. 2001;110(02):103–104. - PubMed
-
- Colletti V, Carner M, Miorelli V, Guida M, Colletti L, Fiorino F. Auditory brainstem implant (ABI): new frontiers in adults and children. Otolaryngol Head Neck Surg. 2005;133(01):126–138. - PubMed
-
- Grayeli A B, Bouccara D, Kalamarides M et al.Auditory brainstem implant in bilateral and completely ossified cochleae. Otol Neurotol. 2003;24(01):79–82. - PubMed
-
- Colletti V, Carner M, Miorelli V, Guida M, Colletti L, Fiorino F G. Cochlear implantation at under 12 months: report on 10 patients. Laryngoscope. 2005;115(03):445–449. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
