

Rapid Neurologic Improvement Predicts Favorable Outcome 90 Days After Thrombectomy in the DEFUSE 3 Study
- PMID: 30932783
- PMCID: PMC6476661
- DOI: 10.1161/STROKEAHA.119.024928
Rapid Neurologic Improvement Predicts Favorable Outcome 90 Days After Thrombectomy in the DEFUSE 3 Study
Abstract
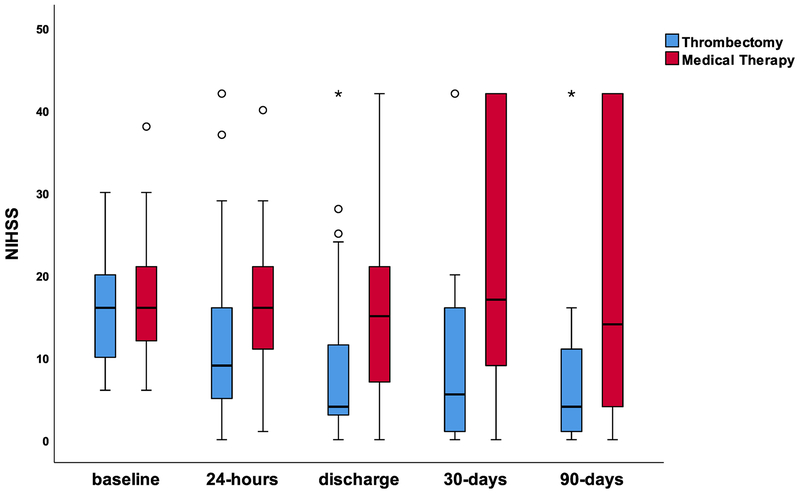
Background and Purpose- Thrombectomy in late time windows leads to improved outcomes in patients with ischemic stroke due to large vessel occlusion. We determined whether patients with rapid neurological improvement (RNI) 24 hours after thrombectomy were more likely to have a favorable clinical outcome in the DEFUSE 3 study (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3). Methods- All patients who underwent thrombectomy in DEFUSE 3 were included. RNI was defined as a reduction of ≥8 on the National Institutes of Health Stroke Scale or National Institutes of Health Stroke Scale zero to one 24 hours after thrombectomy. Clinical outcomes were assessed by an ordinal analysis modified Rankin Scale score and a dichotomous analysis for 90-day independence (modified Rankin Scale score, 0-2). Results- Ninety-one patients in DEFUSE 3 underwent thrombectomy with follow-up data; 31 patients (34%) experienced RNI (RNI+) after thrombectomy and 60 patients (66%) did not (RNI-). Patient demographics and stroke presentation and imaging details were similar between RNI+ and RNI- patients. Reperfusion (Thrombolysis in Cerebral Infarction 2b-3) after thrombectomy was achieved in 26 (84%) RNI+ and 43 (72%) RNI- ( P=0.2). Symptomatic intracranial hemorrhage occurred in no RNI+ and 8% of RNI- patients ( P=0.2). RNI was associated with a favorable modified Rankin Scale shift at day 90 (odds ratio, 3.8; CI, 1.7-8.6; P=0.001) and higher rates of modified Rankin Scale zero to 2 (61% versus 37%; odds ratio, 2.7; CI, 1.1-6.7; P=0.03). Mortality was 3% in RNI+ versus 18% in RNI- ( P=0.05). RNI+ patients had lower median 24-hour National Institutes of Health Stroke Scale (5 [interquartile range (IQR), 1-7] versus 13 [IQR, 7.5-21]; P<0.001), smaller 24-hour infarction volume (21 [IQR, 5-32] versus 65 [IQR, 27-145] mL; P<0.001), and less 24-hour infarct growth (8 [IQR, 1-18] versus 37 [IQR, 16-105] mL; P<0.001) compared with RNI- patients. Hospital stay was shorter in RNI+ (3.7 [IQR, 2.9-7.1] versus 7.4 [IQR, 5.2-12.1] days in RNI-; P<0.001). Conclusions- RNI following thrombectomy correlates with favorable clinical and radiographic outcomes and reduced hospital length of stay. RNI was a favorable prognostic sign following late-window thrombectomy in DEFUSE 3. Clinical Trial Registration- URL: https://www.clinicaltrials.gov . Unique identifier: NCT02586415.
Keywords: demography; endovascular; humans; outcome; reperfusion; stroke; thrombectomy.
Figures
Similar articles
-
Outcomes of Thrombectomy in Transferred Patients With Ischemic Stroke in the Late Window: A Subanalysis From the DEFUSE 3 Trial.JAMA Neurol. 2019 Jun 1;76(6):682-689. doi: 10.1001/jamaneurol.2019.0118. JAMA Neurol. 2019. PMID: 30734042 Free PMC article.
-
Results From DEFUSE 3: Good Collaterals Are Associated With Reduced Ischemic Core Growth but Not Neurologic Outcome.Stroke. 2019 Mar;50(3):632-638. doi: 10.1161/STROKEAHA.118.023407. Stroke. 2019. PMID: 30726184 Free PMC article.
-
Association of Thrombectomy With Stroke Outcomes Among Patient Subgroups: Secondary Analyses of the DEFUSE 3 Randomized Clinical Trial.JAMA Neurol. 2019 Apr 1;76(4):447-453. doi: 10.1001/jamaneurol.2018.4587. JAMA Neurol. 2019. PMID: 30688974 Free PMC article. Clinical Trial.
-
Advanced Neuroimaging in Stroke Patient Selection for Mechanical Thrombectomy.Stroke. 2018 Dec;49(12):3067-3070. doi: 10.1161/STROKEAHA.118.022540. Stroke. 2018. PMID: 30571421
-
Systematic review and meta-analysis of current rates of first pass effect by thrombectomy technique and associations with clinical outcomes.J Neurointerv Surg. 2021 Mar;13(3):212-216. doi: 10.1136/neurintsurg-2020-016869. Epub 2021 Jan 13. J Neurointerv Surg. 2021. PMID: 33441394 Free PMC article.
Cited by
-
Impact of lipid profiles on parenchymal hemorrhage and early outcome after mechanical thrombectomy.Ann Clin Transl Neurol. 2023 Oct;10(10):1714-1724. doi: 10.1002/acn3.51861. Epub 2023 Aug 2. Ann Clin Transl Neurol. 2023. PMID: 37533211 Free PMC article.
-
Time-variant and tissue-level collaterals predict postoperative neurological recovery and clinical outcomes of patients with endovascular thrombectomy.Quant Imaging Med Surg. 2025 May 1;15(5):4085-4100. doi: 10.21037/qims-24-1073. Epub 2025 Apr 28. Quant Imaging Med Surg. 2025. PMID: 40384651 Free PMC article.
-
Association between rehabilitation after reperfusion treatment and in-hospital mortality: Results from a national registry study.Front Neurol. 2022 Sep 14;13:949669. doi: 10.3389/fneur.2022.949669. eCollection 2022. Front Neurol. 2022. PMID: 36188393 Free PMC article.
-
Etiologic and prognostic value of external carotid artery thrombus detection during endovascular therapy for anterior circulation proximal occlusions.Eur J Neurol. 2023 Feb;30(2):380-388. doi: 10.1111/ene.15623. Epub 2022 Nov 20. Eur J Neurol. 2023. PMID: 36325682 Free PMC article.
-
Early Neurological Improvement Predicts Clinical Outcome After Thrombectomy for Distal Medium Vessel Occlusions.Front Neurol. 2022 Mar 7;13:809066. doi: 10.3389/fneur.2022.809066. eCollection 2022. Front Neurol. 2022. PMID: 35321507 Free PMC article.
References
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. The New England journal of medicine. 2015;372:11–20 - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. The New England journal of medicine. 2015;372:1019–1030 - PubMed
-
- Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. The New England journal of medicine. 2015;372:2296–2306 - PubMed
-
- Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. Stent-retriever thrombectomy after intravenous t-pa vs. T-pa alone in stroke. The New England journal of medicine. 2015;372:2285–2295 - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. The New England journal of medicine. 2015;372:1009–1018 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
