

Genome-wide copy number alteration and VEGFA amplification of circulating cell-free DNA as a biomarker in advanced hepatocellular carcinoma patients treated with Sorafenib
- PMID: 30935424
- PMCID: PMC6444867
- DOI: 10.1186/s12885-019-5483-x
Genome-wide copy number alteration and VEGFA amplification of circulating cell-free DNA as a biomarker in advanced hepatocellular carcinoma patients treated with Sorafenib
Abstract
Background: Although sorafenib is the global standard first-line systemic treatment for unresectable hepatocellular carcinoma (HCC), it does not have reliable predictive or prognostic biomarkers. Circulating cell-free DNA (cfDNA) has shown promise as a biomarker for various cancers. We investigated the use of cfDNA to predict clinical outcomes in HCC patients treated with sorafenib.
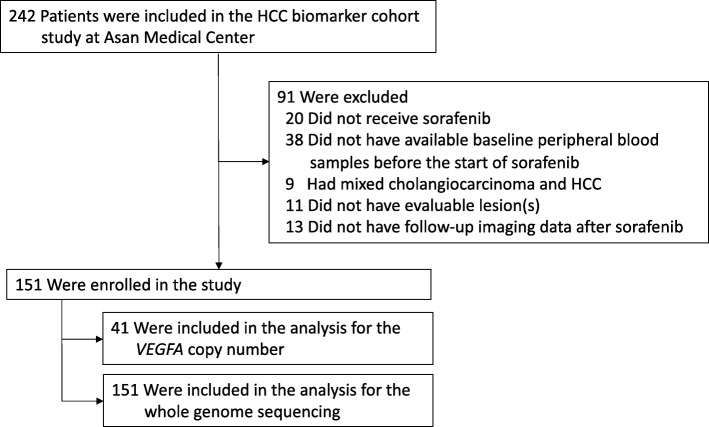
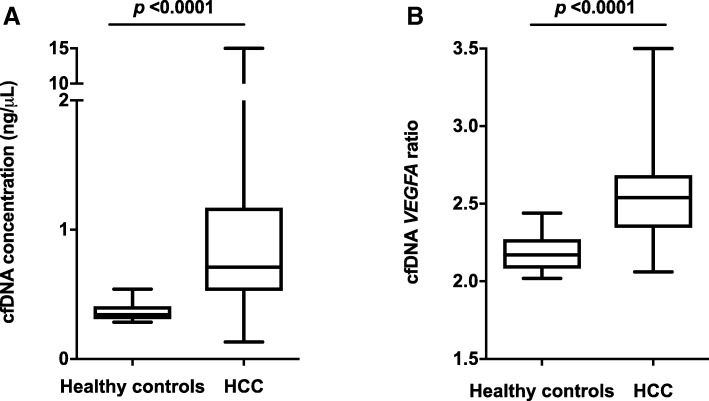
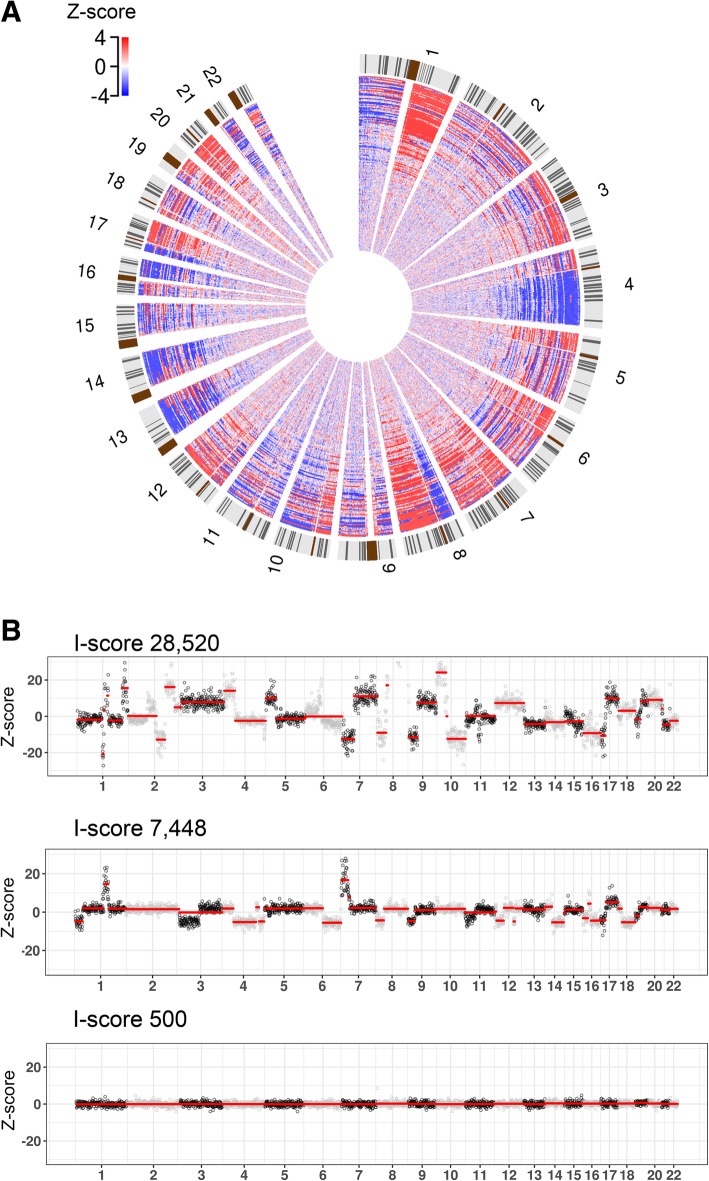
Methods: This prospective biomarker study analyzed plasma cfDNA from 151 HCC patients who received first-line sorafenib and 14 healthy controls. The concentration and VEGFA-to-EIF2C1 ratios (the VEGFA ratio) of cfDNA were measured. Low depth whole-genome sequencing of cfDNA was used to identify genome-wide copy number alteration (CNA), and the I-score was developed to express genomic instability. The I-score was defined as the sum of absolute Z-scores of sequenced reads on each chromosome. The primary aim of this study was to develop cfDNA biomarkers predicting treatment outcomes of sorafenib, and the primary study outcome was the association between biomarkers with treatment efficacy including disease control rate (DCR), time to progression (TTP) and overall survival (OS) in these patients.
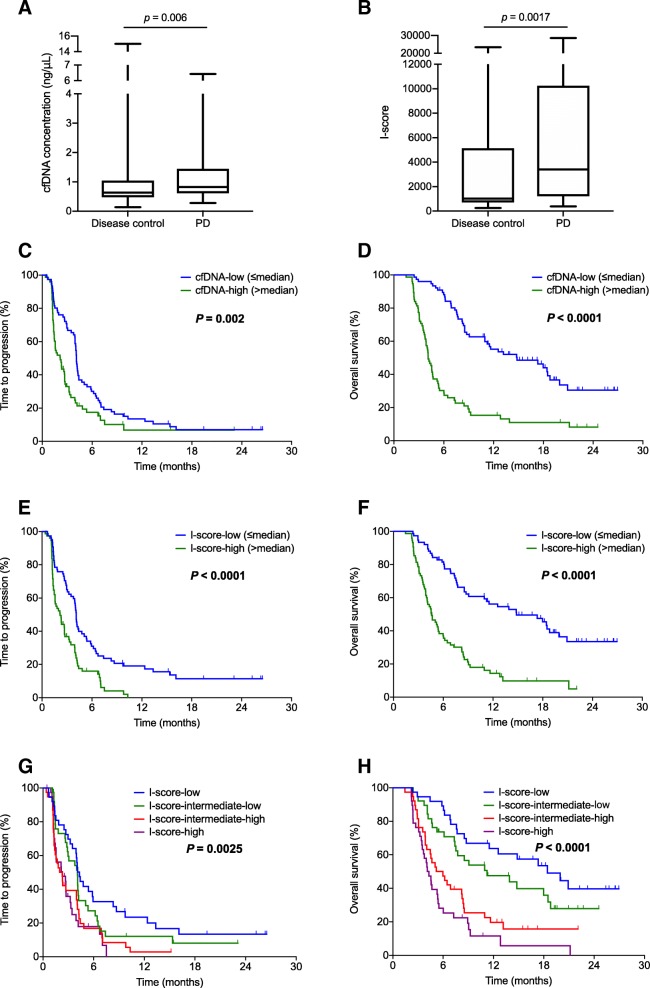
Results: The cfDNA concentrations were significantly higher in HCC patients than in healthy controls (0.71 vs. 0.34 ng/μL; P < 0.0001). Patients who did not achieve disease control with sorafenib had significantly higher cfDNA levels (0.82 vs. 0.63 ng/μL; P = 0.006) and I-scores (3405 vs. 1024; P = 0.0017) than those achieving disease control. The cfDNA-high group had significantly worse TTP (2.2 vs. 4.1 months; HR = 1.71; P = 0.002) and OS (4.1 vs. 14.8 months; HR = 3.50; P < 0.0001) than the cfDNA-low group. The I-score-high group had poorer TTP (2.2 vs. 4.1 months; HR = 2.09; P < 0.0001) and OS (4.6 vs. 14.8 months; HR = 3.35; P < 0.0001). In the multivariable analyses, the cfDNA remained an independent prognostic factor for OS (P < 0.0001), and the I-score for both TTP (P = 0.011) and OS (P = 0.010). The VEGFA ratio was not significantly associated with treatment outcomes.
Conclusion: Pretreatment cfDNA concentration and genome-wide CNA in cfDNA are potential biomarkers predicting outcomes in advanced HCC patients receiving first-line sorafenib.
Keywords: Biomarker; Circulating cell-free DNA; Genome-wide copy number alteration; Hepatocellular carcinoma; Sorafenib; Vascular endothelial growth factor-a.
Conflict of interest statement
Ethics approval and consent to participate
This prospective biomarker study was conducted under approval from the Institutional Review Board (IRB) at Asan Medical Center, Korea. All patients provided written informed consent before study enrollment.
Consent for publication
Not applicable.
Competing interests
EHC, JHJ, and JL are employees of Genome Research Center, Green Cross Genome. All remaining authors declare no actual or potential conflicts of interest.
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. doi: 10.1016/S1470-2045(08)70285-7. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
